
Fillable Printable 57.206 Hcwpep Blank
Fillable Printable 57.206 Hcwpep Blank
57.206 Hcwpep Blank
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
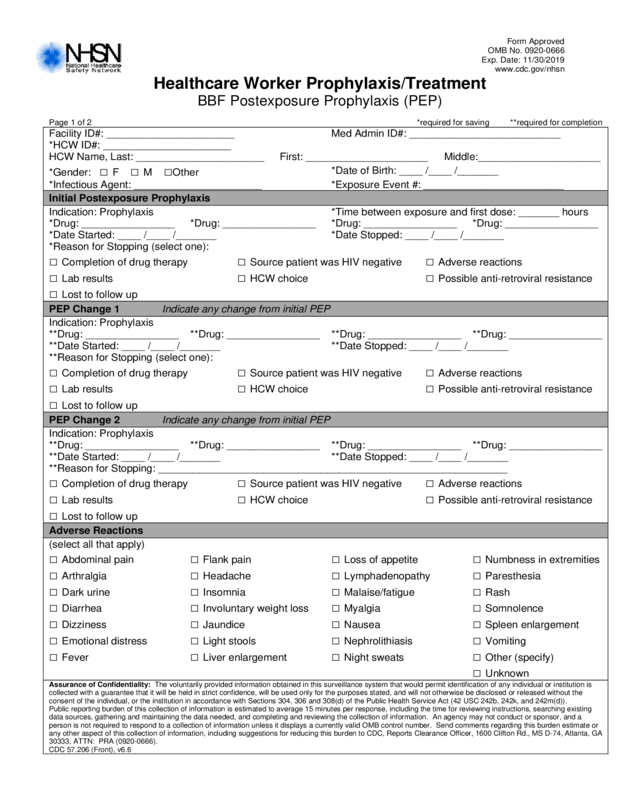
Healthcare Worker Prophyl axis/Treatment
BBF Postexposure Prophylaxis (PEP)
Page 1 of 2 *required for saving **required for completion
Facility ID#: ______________________ Med Admin ID#: __________________________
*HCW ID#: ______________________
HCW Name, Last: ______ ____ ____ _______ _ First: __________ ___________ Middle:_____________________
*Gender: □ F □ M □Other
*Date of Birth: ____ / ____ /_______
*Infectious Agent: ______________________ *Exposure Event #: _________________ _______
Initial Postexposure Prophylaxis
Indication: Prophyl axis *Time between exposure and first dose: _______ hours
*Drug: _________ _______ *Drug: ________________ *Drug: ________________ *Drug: ________________
*Date Started: ____ / ____ /_______ *Date Stoppe d: ____ /____ /_______
*Reason for St oppi ng (select one):
□ Completion of drug therapy □ Source patient was HIV negative □ Adverse reactions
□ Lab results □ HCW choice □ Possible anti-retrov i ral resistance
□ Lost to follow up
PEP Change 1 Indicate any change f rom initial PEP
Indication: Prophyl axis
**Drug: ________ ________ **Drug: ________ ________ **Dr ug: ____________ ____ **Drug: _______________ _
**Date Started: ____ / ____ /_______ **Date Stopped: ____ /____ /_______
**Reason for St oppi ng (select one):
□ Completion of drug therapy □ Source patient was HIV negative □ Adverse reactions
□ Lab results □ HCW choice □ Possible anti-retrov i ral resistance
□ Lost to follow up
PEP Change 2 Indicate any change f rom initial PEP
Indication: Prophyl axis
**Drug: ________ ________ **Drug: ________ ________ **Drug: ____________ ____ **Drug: _______________ _
**Date Started: ____ / ____ /_______ **Date Stopped: ____ /____ /_______
**Reason for Stopping: ____________________________________________________________
□ Completion of drug therapy □ Source patient was HIV negative □ Adverse reactions
□ Lab results □ HCW choice □ Possible anti-retrov i ral resistance
□ Lost to follow up
Adverse Reactions
(select all that appl y)
□ Abdominal pain □ Flank pain □ Loss of appetite □ Numbness in extremities
□ Arthralgia □ Headache □ Lymphadenopathy □ Paresthesia
□ Dark urine □ Insomnia □ Malaise/fatigue □ Rash
□ Diarrhea □ Involuntary weight loss □ Myalgia □ Somnolence
□ Dizziness □ Jaundice □ Nausea □ Spleen enlargement
□ Emotional distress □ Light stools □ Nephrolithiasis □ Vomiting
□ Fever □ Liver enlargement □ Night sweats □ Other (specify)
□ Unknown
Assurance of Confide nt iality: The voluntarily provided information obtained in this surveillance system that would permit identification of any individual or institution is
collected with a guarantee that it will be held in strict confidence, will be used only for the purposes stated, and will not otherwise be disclosed or released without the
consent of the individual, or the institution in accordance with Sections 304, 306 and 308(d) of the Public Health Service Act (42 USC 242b, 242k, and 242m(d)).
Public reporting burden of this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing
data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a
person is not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or
any other aspect of this collection of information, including suggestions for reducing this burden to CDC, Reports Clearance Officer, 1600 Clifton Rd., MS D-74, Atlanta, GA
30333, ATTN: PRA (0920-0666).
CDC 57.206 (Front), v6. 6
Form Approved
OMB No. 0920-0666
Exp. Date: 11/30/2019
www.cdc.gov/nhsn
CDC 57.206 (Back), v6.6
Healthcare Worker Prophylaxis/Treatment
Page 2 of 2
Custom Fields
Label Label
_________________________ ____/____/_____ _______________________ ____/____/_____
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
_________________________ ______________ _______________________ ______________
Comments


