
- Health Care Power of Attorney - South Carolina
- Health Care Power of Attorney - Rhode Island
- Durable Power of Attorney for Health Care - Ohio
- Power of Attorney for Health Care Will to Live Form - Maine
- Durable Power of Attorney for Health Care - Washington
- Power of Attorney for Health Care Will to Live Form - Idaho
Fillable Printable Durable Power of Attorney for Health Care Example - Kansas
Fillable Printable Durable Power of Attorney for Health Care Example - Kansas
Durable Power of Attorney for Health Care Example - Kansas
uT R Ty R T
T T S uT R Ty R T
or
T
T
S T S T SP R
S
P
W
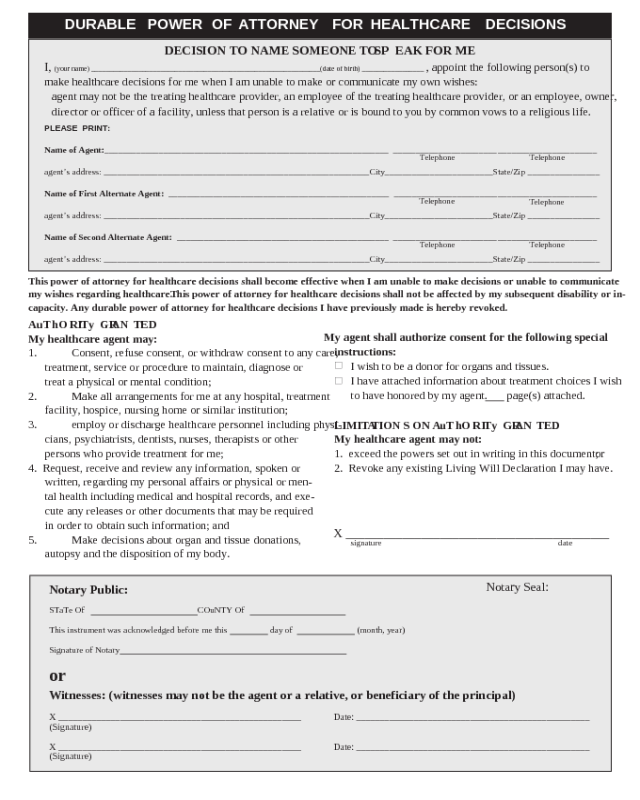
DURABLE
POWER
OF
ATTORNEY
FOR
HEALTHCARE
DECISIONS
DECI ION O NAME OMEONE O EAK FO ME
I,
(your name) _______________________________________________________________ (date of birth) _________________
,
appoint the following person(s) to
make healthcare decisions for me when I am unable to make or communicate my own wishes:
agent may not be the treating healthcare provider, an employee of the treating healthcare provider, or an employee, owner,
director or officer of a facility, unless that person is a relative or is bound to you by common vows to a religious life.
PLEASE PRINT:
Name of Agent:_______________________________________________________________ _______________________ ______________________
agent’s address: ___________________________________________________________City________________________State/Zip ________________
Name of First Alternate Agent: _________________________________________________ _______________________ ______________________
agent’s address: ___________________________________________________________City________________________State/Zip ________________
Name of econd Alternate Agent: _______________________________________________ _______________________ ______________________
agent’s address: ___________________________________________________________City________________________State/Zip ________________
Telephone
Telephone
Telephone
Telephone
Telephone
Telephone
his power of attorney for healthcare decisions shall become effective when I am unable to make decisions or unable to communicate
my wishes regarding healthcare. his power of attorney for healthcare decisions shall not be affected by my subsequent disability or in-
capacity. Any durable power of attorney for healthcare decisions I have previously made is hereby revoked.
A hO I G AN ED
My healthcare agent may:
1. Consent, refuse consent, or withdraw consent to any care,
treatment, service or procedure to maintain, diagnose or
treat a physical or mental condition;
2. Make all arrangements for me at any hospital, treatment
facility, hospice, nursing home or similar institution;
3. employ or discharge healthcare personnel including physi-
cians, psychiatrists, dentists, nurses, therapists or other
persons who provide treatment for me;
4. Request, receive and review any information, spoken or
written, regarding my personal affairs or physical or men-
tal health including medical and hospital records, and exe-
cute any releases or other documents that may be required
in order to obtain such information; and
5. Make decisions about organ and tissue donations,
autopsy and the disposition of my body.
My agent shall authorize consent for the following special
instructions:
■
I wish to be a donor for organs and tissues.
■
I have attached information about treatment choices I wish
to have honored by my agent. page(s) attached.
LIMI A ION ON A hO I G AN ED
My healthcare agent may not:
1. exceed the powers set out in writing in this document;
2. Revoke any existing Living Will Declaration I may have.
X __________________________________________
signature date
Notary Seal:
Notary ublic:
STaTe Of COuNTY Of
This instrument was acknowledged before me this day of (month, year)
Signature of Notary
or
itnesses: (witnesses may not be the agent or a relative, or beneficiary of the principal)
X ___________________________________________________ Date: _________________________________________________
(Signature)
X ___________________________________________________ Date: _________________________________________________
(Signature)


