
- Durable Power of Attorney for Health Care and Living Will
- Washington Durable Power of Attorney for Health Care
- Health Care Power of Attorney Example - South Carolina
- Power of Attorney for Health Care Will to Live Form - Idaho
- Statutory Short Form Power of Attorney for Health Care - Illinois
- Health Care Power of Attorney - Maine
Fillable Printable Durable Power of Attorney for Health Care - Nevada
Fillable Printable Durable Power of Attorney for Health Care - Nevada
Durable Power of Attorney for Health Care - Nevada

DPA.HC (1-02) -1- Principal______
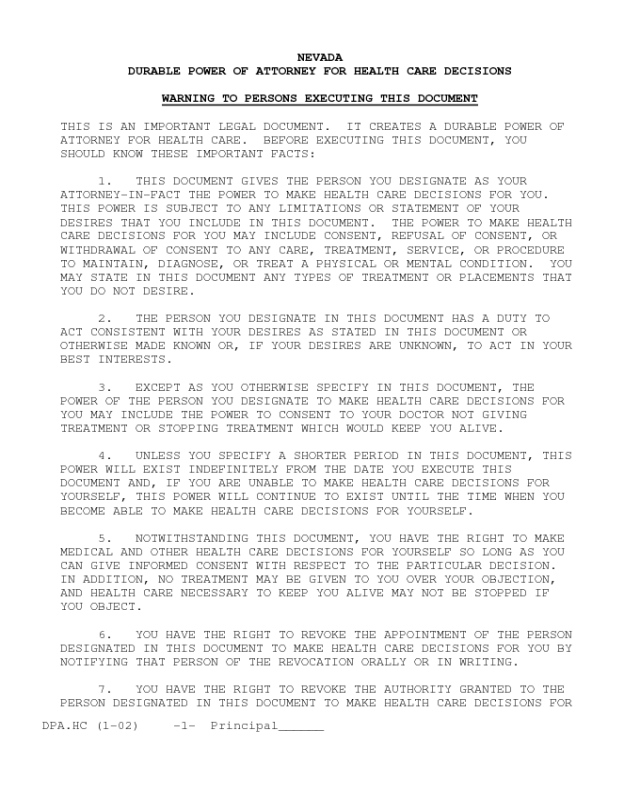
NEVADA
DURABLE POWER OF ATTORNEY FOR HEALTH CARE DECISIONS
WARNING TO PERSONS EXECUTING THIS DOCUMENT
THIS IS AN IMPORTANT LEGAL DOCUMENT. IT CREATES A DURABLE POWER OF
ATTORNEY FOR HEALTH CARE. BEFORE EXECUTING THIS DOCUMENT, YOU
SHOULD KNOW THESE IMPORTANT FACTS:
1. THIS DOCUMENT GIVES THE PERSON YOU DESIGNATE AS YOUR
ATTORNEY-IN-FACT THE POWER TO MAKE HEALTH CARE DECISIONS FOR YOU.
THIS POWER IS SUBJECT TO ANY LIMITATIONS OR STATEMENT OF YOUR
DESIRES THAT YOU INCLUDE IN THIS DOCUMENT. THE POWER TO MAKE HEALTH
CARE DECISIONS FOR YOU MAY INCLUDE CONSENT, REFUSAL OF CONSENT, OR
WITHDRAWAL OF CONSENT TO ANY CARE, TREATMENT, SERVICE, OR PROCEDURE
TO MAINTAIN, DIAGNOSE, OR TREAT A PHYSICAL OR MENTAL CONDITION. YOU
MAY STATE IN THIS DOCUMENT ANY TYPES OF TREATMENT OR PLACEMENTS THAT
YOU DO NOT DESIRE.
2. THE PERSON YOU DESIGNATE IN THIS DOCUMENT HAS A DUTY TO
ACT CONSISTENT WITH YOUR DESIRES AS STATED IN THIS DOCUMENT OR
OTHERWISE MADE KNOWN OR, IF YOUR DESIRES ARE UNKNOWN, TO ACT IN YOUR
BEST INTERESTS.
3. EXCEPT AS YOU OTHERWISE SPECIFY IN THIS DOCUMENT, THE
POWER OF THE PERSON YOU DESIGNATE TO MAKE HEALTH CARE DECISIONS FOR
YOU MAY INCLUDE THE POWER TO CONSENT TO YOUR DOCTOR NOT GIVING
TREATMENT OR STOPPING TREATMENT WHICH WOULD KEEP YOU ALIVE.
4. UNLESS YOU SPECIFY A SHORTER PERIOD IN THIS DOCUMENT, THIS
POWER WILL EXIST INDEFINITELY FROM THE DATE YOU EXECUTE THIS
DOCUMENT AND, IF YOU ARE UNABLE TO MAKE HEALTH CARE DECISIONS FOR
YOURSELF, THIS POWER WILL CONTINUE TO EXIST UNTIL THE TIME WHEN YOU
BECOME ABLE TO MAKE HEALTH CARE DECISIONS FOR YOURSELF.
5. NOTWITHSTANDING THIS DOCUMENT, YOU HAVE THE RIGHT TO MAKE
MEDICAL AND OTHER HEALTH CARE DECISIONS FOR YOURSELF SO LONG AS YOU
CAN GIVE INFORMED CONSENT WITH RESPECT TO THE PARTICULAR DECISION.
IN ADDITION, NO TREATMENT MAY BE GIVEN TO YOU OVER YOUR OBJECTION,
AND HEALTH CARE NECESSARY TO KEEP YOU ALIVE MAY NOT BE STOPPED IF
YOU OBJECT.
6. YOU HAVE THE RIGHT TO REVOKE THE APPOINTMENT OF THE PERSON
DESIGNATED IN THIS DOCUMENT TO MAKE HEALTH CARE DECISIONS FOR YOU BY
NOTIFYING THAT PERSON OF THE REVOCATION ORALLY OR IN WRITING.
7. YOU HAVE THE RIGHT TO REVOKE THE AUTHORITY GRANTED TO THE
PERSON DESIGNATED IN THIS DOCUMENT TO MAKE HEALTH CARE DECISIONS FOR
DPA.HC (1-02) -2- Principal______
YOU BY NOTIFYING THE TREATING PHYSICIAN, HOSPITAL, OR OTHER PROVIDER
OF HEALTH CARE ORALLY OR IN WRITING.
8. THE PERSON DESIGNATED IN THIS DOCUMENT TO MAKE HEALTH CARE
DECISIONS FOR YOU HAS THE RIGHT TO EXAMINE YOUR MEDICAL RECORDS AND
TO CONSENT TO THEIR DISCLOSURE UNLESS YOU LIMIT THIS RIGHT IN THIS
DOCUMENT.
9. THIS DOCUMENT REVOKES ANY PRIOR DURABLE POWER OF ATTORNEY
FOR HEALTH CARE.
10. IF THERE IS ANYTHING IN THIS DOCUMENT THAT YOU DO NOT
UNDERSTAND, YOU SHOULD ASK A LAWYER TO EXPLAIN IT TO YOU.
1. DESIGNATION OF HEALTH CARE AGENT.
I, ________________________________________(insert your name),
do hereby designate and appoint:
Name: _____________________________________________________
Address: __________________________________________________
__________________________________________________
Phone: (____)________________
as my attorney-in-fact to make health care decisions for me as
authorized in this document.
(Insert the name and address of the person you wish to
designate as your attorney-in-fact to make health care decision for
you. Unless the person is also your spouse, legal guardian or the
person most closely related to you by blood, none of the following
may be designated as your attorney-in-fact: (1) your treating
provider of health care, (2) an employee of your treating provider
of health care, (3) an operator of a health care facility, or (4) an
employee of an operator of a health care facility.)
2. CREATION OF DURABLE POWER OF ATTORNEY FOR HEALTH CARE.
By this document I intend to create a durable power of attorney
by appointing the person designated above to make health care
decisions for me. This power of attorney shall not be affected by
my subsequent incapacity.
3. GENERAL STATEMENT OF AUTHORITY GRANTED.
In the event that I am incapable of giving informed consent
DPA.HC (1-02) -3- Principal______
with respect to health care decisions, I hereby grant to the
attorney-in-fact named above full power and authority to make health
care decisions for me before, or after my death, including:
consent, refusal of consent, or withdrawal of consent to any care,
treatment,
service, or procedure to maintain, diagnose, or treat a physical or
mental condition, subject only to the limitations and special
provision, if any, set forth in paragraph 4 or 6.
4. SPECIAL PROVISIONS AND LIMITATIONS.
(Your attorney-in-fact is not permitted to consent to any of
the following: commitment to or placement in a mental health
treatment facility, convulsive treatment, psycho surgery,
sterilization, or abortion. If there are any other types of
treatment or placement that you do not want your attorney-in-fact's
authority to give consent for or other restrictions you wish to
place on his or her attorney-in-fact's authority, you should list
them in the space below. If you do not write any limitations, your
attorney-in-fact will have the broad powers to make health care
decisions on your behalf which are set forth in paragraph 3, except
to the extent that there are limits provided by law.)
In exercising the authority under this durable power of
attorney for health care, the authority of my attorney-in-fact is
subject to the following special provisions and limitations:
____________________________________________________________________
_
____________________________________________________________________
_
5. DURATION.
I understand that this power of attorney will exist
indefinitely from the date I execute this document unless I
establish a shorter time. If I am unable to make health care
decisions for myself when this power of attorney expires, the
authority I have granted my attorney-in-fact will continue to exist
until the time when I become able to make health care decisions for
myself.
(IF APPLICABLE)
I wish to have this power of attorney end on the following
date: _________________________________.
6. STATEMENT OF DESIRES.
DPA.HC (1-02) -4- Principal______
(With respect to decisions to withhold or withdraw life-
sustaining treatment, your attorney-in-fact must make health care
decisions that are consistent with your known desires. You can, but
are not required to, indicate your desires below. If your desires
are unknown, your attorney-in-fact has the duty to act in your best
interests; and, under some circumstances, a judicial proceeding may
be necessary so that a court can determine the health care decision
that is in your best interests. If you wish to indicate your
desires, you may INITIAL the statement or statements that reflect
your desires and/or write your own statements in the space below.)
(IF THE STATEMENT REFLECTS YOUR DESIRES, INITIAL THE
BOX NEXT TO THE STATEMENT.)
(1) I desire that my life be prolonged to the greatest
extent possible, without regard to my condition, the
chances I have for recovery or long term survival,
or the cost of the procedures. [_________]
(2) If I am in a coma which my doctors have
reasonably concluded is irreversible, I desire
that life-sustaining or prolonging treatments
not be used. (Also should utilize provisions of
NRS 449.535 to 449.690, inclusive, if this
subparagraph is initialed.) [_________]
(3) If I have an incurable or terminal condition
or illness and no reasonable hope of long term
recovery or survival, I desire that life-
sustaining or prolonging treatments not be
used. (Also should utilize provisions of
NRS 449.535 to 449.690, inclusive, if this
subparagraph is initialed.) [_________]
(4) Withholding or withdrawal of artificial
nutrition and hydration may result in death
by starvation or dehydration. I want to
receive or continue receiving artificial
nutrition and hydration by way of the
gastro-intestinal tract after all other
treatment is withheld. [_________]
(5) Except as set forth in Paragraph (2)
and/or (3) above, I do not desire treatment
to be provided and/or continued if the burdens
of the treatment outweigh the expected benefits.
My attorney-in-fact is to consider the relief of
DPA.HC (1-02) -5- Principal______
suffering, the preservation or restoration of
functioning, and the quality as well as the
extent of the possible extension of my life. [_________]
(6) I do not desire treatment to be provided
and/or continued if the burdens of the treatment
outweigh the expected benefits. My attorney-in
-fact is to consider the relief of suffering, the
preservation or restoration of functioning, and
the quality as well as the extent of the possible
extension of my life. [_________]
(7) If any of my tissues or organs are sound
and would be of value, I freely give my per-
mission for such donation pursuant to the
Uniform Anatomical Gift Act (NRS 451.500) for
the following purposes:
(a) For transplant to other people. [__________]
(b) For transplant to family, only. [__________]
(c) For medical research. [__________]
(8) I want the financial cost of my medical
treatment to be taken into account and weighed
against the likelihood that the treatment will
achieve the goals that I have initialed above. [_________]
(9) If I am disabled, but not in need of nursing
home care, then I direct my attorney-in-fact to
obtain an individualized care plan for me which
is to be prepared by a geriatric care manager
within 60 days of my disability. In making said
plan, I direct that the plan be developed in a
manner so that I can be maintained in the least
restrictive environment. [_________]
(10) If a guardian is appointed of my person and/
or estate, by a court of competent jurisdiction,
then I direct my attorney-in-fact to submit this
Durable Power of Attorney for Health Care Decisions
to said court. I then request that said court
implement my directives contained herein and that
the court direct, by its order, that my designated
attorney-in-fact is to continue to make my health
care and placement decisions in accordance with
this document, even if my attorney-in-fact is not
a Nevada resident. [_________]
DPA.HC (1-02) -6- Principal______
(11) If I am diagnosed as having dementia or the
Alzheimer's type or other dementia that is deemed
by best available medical knowledge to be
progressive and irreversible, and I no longer have
decision-making capacity, I desire that I be allowed
to die of natural causes such as pneumonia or
dehydration if I become ill or fail to take in
enough fluids by mouth. [_________]
(12) It is my desire to be comfortable. If I
cannot communicate with my Doctor, family or
friends, then I want my Attorney-in-fact, family
and friends to know the following:
(a) I ask that medical treatment to alleviate
pain, to provide comfort, and to mitigate
suffering be provided so that I may be as
free of pain and suffering as possible.
When the circumstances are appropriate, and
in accordance with my wishes as I have
expressed them, such pain relief may be
authorized even though its use may lead
to physical damage, addiction, or even
hasten the moment of (but not intentionally
cause) my death. [_________]
(b) If my temperature is above normal, I
want a cool moist cloth put on my head. [_________]
(c) I want my mouth and lips kept moist. [_________]
(d) I need to be kept fresh and clean at
all times. I wish to have warm baths
often or warm showers, if I am stable
enough for a shower. [_________]
(e) I desire to be massaged with or without
warm oils as often as you think will help
maintain my skin integrity and provide
for my comfort. [_________]
(f) I want to have my favorite types of
music played when possible. [_________]
(g) I want my personal care such as
nail clipping, hair combing, and teeth
brushing and shaving as long as they do
DPA.HC (1-02) -7- Principal______
not cause me pain. [_________]
(h) I want to have religious readings
read to me when I am near death. [_________]
(i) I want to have my favorite poems
read to me from time to time. [_________]
(j) Please arrange for family pictures to
be placed in my room. [_________]
(13) I hope my family and friends would
consider that:
(a) I enjoy your company and want you
with me when possible. I desire that
one of you stay with me when it seems
that my death may be imminent. [_________]
(b) Please continue to talk to me about
daily happenings and events, even if you
think I don’t understand, because I might
be able to understand. [_________]
(c) Please don’t be afraid to hold my
hand or hug me. [_________]
(d) Please tell the members of my church
or synagogue I am sick and ask them to
pray for me and visit me. [_________]
(e) Please maintain a cheerful atmosphere
around me. [_________]
(f) Please place pictures of my loved
ones in my room, near my bed, or near
the place I sit during the day. [_________]
(g) My clothes and bed linens are to be
kept clean, and they are to be changed
as soon as possible, if they have been
soiled. [_________]
(h) If at all possible, allow me to die
in my home. [_________]
(i) Please arrange for me to watch on
television, or listen to my favorite
sports events. [_________]
DPA.HC (1-02) -8- Principal______
(j) Let me enjoy the outdoors as often
as possible by letting me spend time
in my yard, garden and other appropriate
outdoor places, even if it causes slight
discomfort to either you or me. [_________]
(14) I want my care to be provided in a manner
that promotes palliative care as set forth on
Attachment 1. [_________]
OTHER OR ADDITIONAL STATEMENTS OF DESIRES:
____________________________________________________________________
_
____________________________________________________________________
_
____________________________________________________________________
_
7. It is my intention that this instrument serve both as a
self-executing document and as a delegation of power to my attorney-
in-fact. This document shall be deemed an exercise of all rights
that I may have under the United States Constitution, the
Constitution of Nevada, and any other relevant state and federal
laws, rules, regulations and decisions, to refuse medical treatment.
8. I desire that my wishes be carried out through the
authority given to my attorney-in-fact by this document despite any
contrary feelings, beliefs or opinions of other members of my
family, relatives or friends.
9. I realize that the situations described in this document
are subject to various interpretations, and I am confident that the
person(s) named as my attorney-in-fact will exercise the judgment
that I myself would exercise if competent.
10. If my attorney-in-fact or my alternate attorney(s) in fact
is unavailable, I nevertheless request that my instructions and
preferences in this document be observed.
11. DESIGNATION OF ALTERNATE ATTORNEY-IN-FACT.
(You are not required to designate any alternative attorney-in-
fact but you may do so. Any alternative attorney-in-fact you
DPA.HC (1-02) -9- Principal______
designate will be able to make the same health care decisions as the
attorney-in-fact designated in paragraph 1, page 2, in the event
that he or she is unable or unwilling to act as your attorney-in-
fact. Also, if the attorney-in-fact designated in paragraph 1 is
your spouse, his or her designation as your attorney-in-fact is
automatically revoked by law if your marriage is dissolved.)
If the person designated in paragraph 1 as my attorney-in-fact
is unable to make health care decisions for me, then I designate the
following persons to serve as my attorney-in-fact to make health
care decisions for me as authorized in this document, such persons
to serve in the order listed below:
A. First Alternative Attorney-in-fact
Name: _____________________________________________________
Address: __________________________________________________
__________________________________________________
Phone: (____)________________
B. Second Alternative Attorney-in-fact
Name: _____________________________________________________
Address: __________________________________________________
__________________________________________________
Phone: (____)________________
12. PRIOR DESIGNATIONS REVOKED.
I revoke any prior durable power of attorney for health care.
However, this shall not be construed as a revocation of any durable
power of attorney I may have made for the management of my business
and/or personal affairs.
13. WAIVER OF CONFLICT OF INTEREST.
If my designated attorney-in-fact or if any alternate
designated attorney-in-fact is my spouse or is one of my children
then in that event I waive any conflict of interest that said spouse
or child may have in carrying out the provisions of this Durable
Power of Attorney for Health Care, by reason of the fact that said

DPA.HC (1-02) -10- Principal______
spouse or child may be a recipient of my estate whether by Will, the
laws of intestate succession or pursuant to a Trust or other
arrangement.
(YOU MUST DATE AND SIGN THIS POWER OF ATTORNEY)
I sign my name to this Durable Power of Attorney For Health
Care on:
______________________, 200__ at __________________________________
(date) (city and state)
Signature: _____________________________________
Print Name: _____________________________________
Address: _____________________________________
Town, State, Zip: _____________________________________
Telephone number: ( )
Social Security number: _____________________________________
(THIS POWER OF ATTORNEY WILL NOT BE VALID FOR MAKING HEALTH
CARE DECISIONS UNLESS IT IS EITHER (1) SIGNED BY AT LEAST TWO
QUALIFIED WITNESSES WHO ARE PERSONALLY KNOWN TO YOU AND WHO ARE
PRESENT WHEN YOU SIGN OR ACKNOWLEDGE YOUR SIGNATURE, OR (2)
ACKNOWLEDGED BEFORE A NOTARY PUBLIC.)
CERTIFICATE OF ACKNOWLEDGMENT OF NOTARY PUBLIC
STATE OF NEVADA )
) ss.
COUNTY OF WASHOE )
On this _____ day of ______________, in the year 200__, before
me,___________________________, (here insert name of Notary Public)
personally appeared __________________________________, (here insert
name of principal) personally known to me (or proved to me on the
basis of satisfactory evidence) to be the person who executed the
above instrument, and acknowledged to me that he or she executed the
same for purposes stated therein. I declare under penalty of
perjury that the person whose name is ascribed to this instrument
appears to be of sound mind and under no duress, fraud, or undue
influence.
________________________________

DPA.HC (1-02) -11- Principal______
NOTARY PUBLIC in and for said
County and State.
COPIES: You should retain an executed copy of this document and
give one to your attorney-in-fact. The power of attorney
should be available so a copy may be given to your
providers of health care.


