
Fillable Printable Form 800-053-000
Fillable Printable Form 800-053-000
Form 800-053-000

F800-053-000 Cover letter 5-2011
STATE OF WASHINGTON
DEPARTMENT OF LABOR AND INDUSTRIES
Crime Victims Compensation Progra m
PO Box 44520 •Olympia, Washington 98504-4520
Dear Provider:
If you choose to become an established provider with us, please complete the enclosed
provider application and return it to us at your earliest convenience. Upon registration,
you will receive your provider account number and a packet of information related to
billing our program for your services. We have published a mental health fee schedule
which is available on our website, www.CrimeVictims.Lni.wa.gov. If you have any
questions related to our reimbursement rate you may contact our toll free number.
The Crime Victims Compensation Program (CVCP) is currently reimbursing providers a
percentage of the billing rates used by the Department of Labor and Industries. Our
program is the last payer of benefits. Crime victims must first use any private or public
insurance they have before the CVCP can pay.
If you are currently treating a crime victim with an allowed claim and choose not to
conduct further business with us, you cannot bill the victim for services you have
provided thus far. To be paid for treatment provided to date, you will need to complete
the enclosed provider application agreement and submit it along with your bills to the
CVCP for payment consideration. We will assign a provider account number for bill
processing purposes. After the bills have been processed and you receive your remittance
advice, you may contact us to terminate your account.
If at any time you decide not to accept crime victims as patients, please refer them to our
toll free number (1-800-762-3716) for a listing of CVC registered providers located in
their area.
Sincerely,
The Crime Victims Compensation Program
F800-053-000 Provider Application & Notice 6-2009
MASTER LEVEL COUNSELOR
APPLICATION INSTRUCTIONS
NOTICE:
Each applicant must complete an application. A number will be issued to each individual provider.
If additional copies are needed, copy all portions of the application from the internet or call (360) 902-5377.
Photo copies can be made of this application for completion.
SECTION I: TO BE COMPLETED BY ALL PROVIDERS
Enter the Tax Payer Identification Number (EIN or SSN). The number you will use to report earnings to the
IRS - This must match the information on the W-9.
SECTION II: TO BE COMPLETED BY ALL PROVIDERS
A.
Administrative Information
1.Enter the name of the business you wish to submit your bills and have your account set up as, (DBA).
2.Enter the phone number of the business.
2a. Enter the fax number of the business.
3.Enter the billing address as it appears on your bills submitted to Crime Victims Compensation Program and where payments
should be mailed.
4.Enter the physical address of the business.
5.Enter the contact person's name – person who can answer questions regarding your bills or your account.
6.Enter the billing phone number where we may call to ask questions regarding your bills or your account.
7.If you will be attached to a group, please provide group number (for billing purposes).
B.
Individual or Organization Information – Complete all applicable information
1.Enter the name of the individual or organization providing services to injured workers.
2.Enter the type of service(s) provided.
3.Enter your license, certification or registration number.
4.Enter the date the license, certification or registration was issued (month, day and year).
ATTACH COPY
5.Enter the date the license, certification or registration will expire (month, day and year).
6.Enter the state where the license, certification or registration was issu ed.
C.
National Provider Identifier (NPI) Information
1.Enter the individual or organization name.
2.If application is for a subpart, enter subpart name.
3.Check one. Type I – individual counselor
Type II – mental health clinics.
4.Enter the address associated with the NPI number you have provided.
5.Enter the NPI 10-digit identifier.
6.If application is for a subpart, enter the subpart NPI 10-digit identifier.
7.Enter the taxonomy codes of the individual, organization or subpart. If more than six, please list on a separate sheet of paper.
* Each January the Internal Revenue Service requires us to send a completed Form 1099 MISC reporting payments of
$600.00 or more made to a Federal Tax Identification Number (EIN or SSN) during the last calendar year. If you received
payments from more than one department program, you may receive more than one Form 1099 Misc.
Please Do Not Forget To Read and Sign The "Provider Agreement”
F800-053-000 Provider Application & Notice 6-2009
Master Level Counselor
Provider Account Application
Return To:
Provider Registration
Crime Victims Compensation Program
Department of Labor and Industries
PO Box 44520
Olympia WA 98504-4520
I.TAX REPORTING INFORMATION
A.Administrative Information
1.Business name (as you wish to submit your bills and have your account set up, DBA) 2.Business phone# 2a. Business FAX#
3.Billing address (as it appears on your bills submitted to CVC and where payments should be mailed) 4.Business address (the physical location of the business)
5.Contact person’s name
6.
Billing phone# (where we may call regarding your account/bills)
7.CVC group payee provider #
B.Individual or Organization Information – Attach copy of current license
1.Provider’s name (Last, First, MI) 2.Specialty / Services provided
3.Professional license/certification/registration number 4.License issue date 5. License expiration date6. State where issued
C. National Provider Identifier (NPI) Information
1. Individual or Organization name 2. If for Subpart, provide Subpart name 3. Please check one
Type I Individual Type II Organization
4. NPI address
5. NPI 10-digit Identifier 6. If for Subpart, provider Subpart NPI 10-digit identifier
__ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
7. Taxonomy Codes
__ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
__ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
(Please type or print clearly on all sections)
Please
check:
New Provider
Address Updates for Reactivation of Provider Account
Tax ID Change – Effective Date _______________
Required
(360) 902-5377 FAX (360) 902-5333
Internet address: //www.lni.wa.gov/FormPub
Tax Payer Identification Number (EIN or SSN)
THIS NUMBER MUST MATCH THE W-9 FORM YOU SUBMIT
Unless otherwise notified, your claims
related correspondence will go to your
business (physical) address.
Please check if you would like all
mail to go to the billing address.
II.ACCOUNT AND BI LLING INFORMATION
*****
Mental health counselors must have a master’s degree in a field of study related to me ntal health services
including, but not limited to, social work, marriage and family therapy or mental health counseling.
F800-053-000 Provider Application & Notice 6-2009
PROVIDER APPLICATION
The Crime Victims Compensation Program (CVC) is authorized by Washington State law, Title 7, Chapter 68, Revised Code of Washington
(RCW), and is administered by the Department of Labor and Industries. Health care and other services are provided to CVC clients pursuant to
Title 7, Chapter 68 RCW, Washington Administrative Code (WAC) Chapters 296-30, and 296-31, and policies adopted by the department,
including medical coverage decisions. To qualify for payment, a provider must have an active provider account number assigned by CVC.
To receive a provider account number, the provider must submit a signed CVC Provider Application to CVC, including all required supporting
information. For group practices, a separate Provider Application is required for each
provider who will be providing services to CVC clients.
The following information must be submitte d with the Provider Applic ation, a:
•current copy of the provider's current professional license, certification or registration. Master level counselors must
include a copy of academic degree;
•completed W-9 Form.
A provider's account number will become inactive if CVC does not receive any bills from the provider for a consecutive 18-month period. If the
provider's account becomes inactive, the provider must reactivate the account prior to submitting bills by calling the CVC Provider Registration
Section at 360-902-5377. A new W-9 Form is needed to reactivate an account, only if information on that form has changed. Providers with
inactive accounts will not automatically receive department publications, such as Provider Bulletins, Provider Updates, rules. Issuance
ofa
provider number does not guarantee that all services billed by a provider will be paid by CVC. The department will purchase only
covered services, provided by covered professionals.
The provider agrees:
1.To meet and maintain all applicable state and/or federal licensing, certification or registration requirements to assure the department of the
provider's qualifications to perform services.
2.To comply with Washington State Law Title 7, Chapter 68 RCW, and WACs, including but not limited to, Chapters 296-30, and 296-31, and
policies adopted by the department, including fee schedules and medical coverage decisions.
3.That providing services to or filing an application for benefits on behalf of a crime victim who is covered under the department's jurisdiction,
constitutes acceptance of the requirements of Title 7, Chapter 68 RCW, and WACs, including but not limited to, Chapters 296-30, and
296-31, and policies adopted by the department, including fee schedules and medical coverage decisions.
4. To bill CVC the provider’s usual and customary chargesfor services rendered to CVC clients as required by Washington State law.
5.To bill primary or public insurance prior to billing CVC.
6.To accept the department's payment after primary or public insurance has been billed as complete renumeration for services provided to the
CVC client as required by Washington State law. The provider agrees not to bill a CVC client for:
a)services covered by CVC which are related to the crime victim’s claim.
b)the difference between the billed and paid charges; or
c)the difference between the provider's customary fee and the department's fee schedule.
In the event a provider believes additional funds are due, the provider may submit a Provider's Request for Adjustment Form to the
department for consideration in accordance with the instructions contained on the Remittance Advice.
7.That if the provider receives payment from the department in error or in excess of the amount properly due under the applicable rules and
procedures the provider will promptly return to the department any excess monies received. The department may audit the provider's records
to determine compliance with the rules and regulations of the department as provided in Washington State law.
8.To maintain documentation and records for a minimum of five years to support the services and levels of services billed. The provider agrees
that these records and supportive materials will be made available to the department upon request as provided in Washington State law.
9.To notify CVC immediately of any changes to information in this application or provider status (e.g., federal tax identification number,
ownership, incorporation, address, etc.). A change in ownership or fede r al tax ID numbe r may require a new provider account number
A provider will be held to all the terms of this application even though a third party may be involved in billing claims to the
department. The
department reserves the right to deny, revoke, suspend or condition a provider's authorization to treat CVC clients in accordance with Washington
law.
Provider's Statement of Agreement
I (the provider), _____________________________________, (print or type) agree to abide by the terms of this application and by all applicable
federal and Washington State statutes, rules and policies. I have enclosed with my application all
required supporting information to establish a
provider account, including: a current copy of my current license, certification or registration (if I am required to be licensed, certified or
registered by my state licensing authority); and a completed W-9 Form.
Date Title Signature
Statewide Payee Registration for
Washington StateDepartment of Labor and Industries
STEP 1: Is this a NEW registration or CHANGE to an existing registration (check one)?
NEW REGISTRATION― complete the ENTIREform (STEPS 1 ― 6)
EXISTING REGISTRATION – comp lete t he ENTIREform (STEPS 1 – 6) and check below what is updated:
Adding a New Provider Name/DBA Address Contact Information EmailPayment Options
Direct Deposit Additional Information
If you know your Statewide Vendor Number, enter it here:
SWV
STEP 2: Enter information about the payee and contact person
Legal Name (a s show n on your income tax ret urn)
SSN OR EIN
Busines s Nam e, if dif f er e nt from Lega l Na m e abov e – e.g. Doing Busi ne s s As (DBA) Name
Contact Person
PaymentAddress(where payme nts wil l be sent)
Contact Telephone Num ber
City, Sta t e, and Zip Code
Contact Fa x Number
Email to recei v e St ate wi de Ve ndor Num be r a nd payment noti f ic ations
For L&I Use Only:
2350 / MIPS / O /
Type of Busine s s
L&I #/ System / Ownership / L&I Provider #
STEP 3: Select Payment Option:
Direct Deposit to bank (recommended)
Check in US mail (terminates any previous banking information on file)
If dir e ct deposit is checked, complete STEP 4.
STEP 4: For Direct Deposit, complete all fields below and sign
Financial Instit ution Name – must be a US institution
Financial Instit ution Phone Number
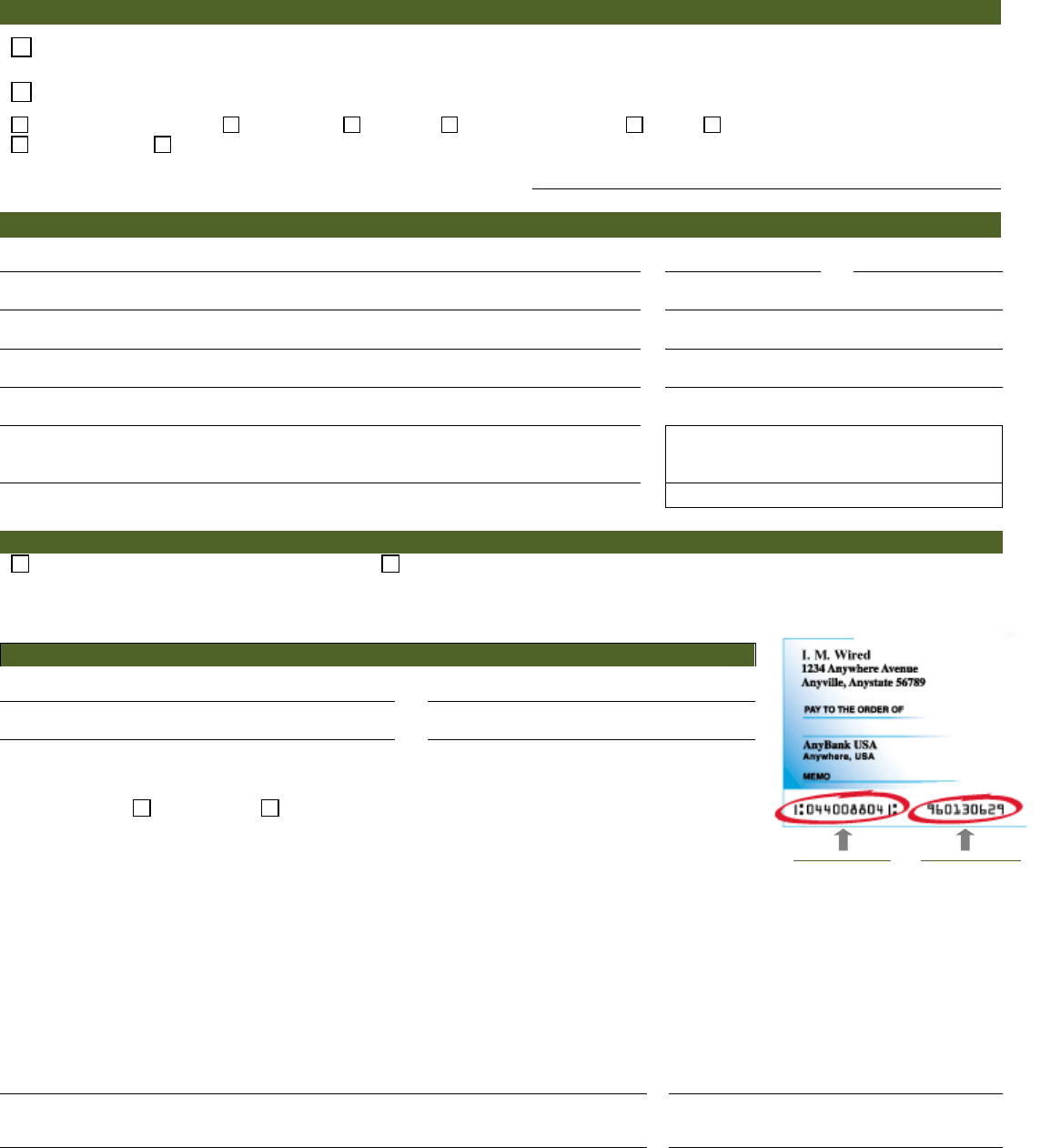
Routing Numbe r – see example at right
Account Numbe r – see example at right
In addition to providing your banking information on this form, you may attach a voide d che ck .
Account Type: Checking or Savings (Checking will be used if neither box is marked.)
Aut
horization for Direct Deposit:
I hereby authorize and request the Consolidated Technology Services (CTS) and the Office of the State Treasurer (OST)
to initiate credit entries for payee pay ments to the account indicated above, and the financial institution named above is
authorized to credit such account. I agree to abide by the National Automated Clearing House Association (NACHA) rules
with regard to these entries. Pursuant to the NACHA rules, CTS and OST may initiate a reversing entry to recall a
duplicate or erroneous entry that theypreviously initiated. I understand that if a reversal action is required, CTS will notify
this office of the error and the reason for the reversal. This authority will continue until such time CTS and OST have had
a reasonable opportunity to act upon written request to terminate or change the direct deposit service initiated herein.
Authorized Representative (Please Print)
Title
SI GNA T U R E of Aut hor ized R epresentat ive
Date
Page 1 of 2
Routing Number
(Nine Digits)
Account Number
can vary in length
Continue to STEP 5
F800-065-000 Substitute Statewide Payee and W-902-2016
STEP 5: REQUIRED – Completeand sign the Reques t for Taxpaye r Identification Number (W-9)
Substitute
Form
W-9
Request for Taxpayer
Identification Number and Certification
1.Legal Name (as shown on your income tax return)
2.Business Name, if different from Legal Name above – eg. Doing Business As (DBA) Name
3.Check ONLY ONE box below (see W-9 instructions for additional information)
Individual or
Sole Proprietor
LLC filing as a sole
proprietor
Partnership
Corporation
S-Corp
LLC filing as
Corporation
LLC filing as
Partnership
LLC filing as S-Corp
Non Profit Organization
Volunteer
Board /Committee
Member
Local Government
State Government
Federal Government
(including tribal)
Tax-exempt organization
Trust/Estate
4.For Corporation, S-Corp, Partnership or LLC, check one box below if applicable:
Medical Attorney/Legal
5.If exempt from backup withholding, check here:(See instructions for W-9 to determine if you are exempt from backup withholding.)
6.Ad d ress (n u mber, street, and apt. or suite no.)
Department of Labor and Industries
Attn: Provider Credentialing and Compliance
PO Box 44261
Olympia Wa98504-4261
7.Cit y, State, and ZIP code
8.Taxpayer Identifi cation Number (TIN)
Enter your EIN ORSSN in the appropriate box to the right (do not enter both)
For individuals, this is your soc i al security number (SSN).
For other entities, it is your empl oyer identification number (EIN).
N
OTE: The EIN or SSN must match the Legal Nameas reported to the IRS. For a resident alien, sole
proprietor, or disregarded ent i ty , or to find out how to get a Taxpayer Identificati on Number, see the W9
Instructions.If the account is in more than one name, see the W9 Instructions for gui del i nes on whose
number to enter.
Social security number
-
-
Employer ident ification number
-
9.Certification
Under penalty of perjury, I certify that:
•
The number shown on this form is my correct taxpayer identification number (or I am waiting for a number to be issued to me), and
•
I am not subject to backup withholding because: (a) I am exempt from backup withholding, or (b) I have not been notified by the
Internal Revenue Service (IRS) that I am subject to backup withholding as a resultof a failure to report all interest or dividends, or
(c) the IRS has notified me that I am no longer subject to backup withholding, and
•
I am a U.S. person (including a U.S. resident alien).
(For additional information about the W-9 see the W-9 Instructions.)
SIGNATURE of U.S. PERSON
Date
STEP 6: Submit to ONE of the following
For Medical Provider
Provider Account Application & Pay Hold Releases:
FAX:360-902-4484
Provider Network Application (WPA):
FAX:360-902-4563
Crime VictimsCompensation:
FAX: 360-902-5333
Or mail to:
Provider Credentialing & Compliance
PO Box 44261
Olympia, WA 98504-4261
For quest ions cont ac t Prov ider Credent i a l ing: 3 60-902-5140and select optio n 4
Page 2 of 2
F800-065-000 Substitute Statewide Payee and W-902-2016
Instructions f or t he St a t ewidePayee Regi s tr a t ion Form
The term ‘payee’ refers to an individual or business that received payments from the State of
W ashington. This form is intended to be used for payees to register with the State of Washington,
indicate how they would like to receive payments, and change their registration information.
For prompt payment, it is important that we receive complete and accurate information. We must
return any form tha t is not com pl ete, so please be sure to read and follow these i nstructions
carefully.
Step 1: Is this a new regis tration or a change to an existing registration?
Select NEW REGISTRATION if:
•You have never completed the Statewide Payee Registration Form.
•You are changing the legal name of a payee already registered.
•You are changing the EIN (Employer Identification Number) or SSN (Social Security
Number) of a payee already registered
•You are changing the reporting type (sole proprietor, corporation, etc) on an existing
registration.
Select CHANGE TO EXISTING REGISTRAT ION for all other changes to an exi st ing
registration, and check the items that have changed. Be sure toCOMPLETE the ENTIRE
form, even if you are only changing one item. This will help us keep your account up to date
and accurate. If you know your SWVnumber, please enter it on the form.
Step 2: Payee & contact information
Legal name of payee – enter the name as it appears on federal tax forms.
Business name– “doing business as” name. Enter only if different from legal name.
Paymentaddress – enter the PO Box or street address where you want information sent to
you. If you choose to have checks mailed to you, this is the address where they will be sent.
Email for contact person - enter the email address we should use to communicate with you
about your registration and your payments. We will use the email address to:
•Notify you when your account has been set up.
•Notify you when changes you submitted have been made.
•Notify you when your payment has been processed, if you have signed up for direct
deposit.
Type ofbusiness– enter the primary occupation of the payee.
SSNor EIN– enter the SSNor EIN you use with the IRS for the legal name entered.
Contact person –the per son w ecan contact with questions about your registration.
Contact telephone number–telep ho ne number of the con tact person.
Contact fax number – fax number of the contact person.
NOTE: For larger organizations we recommend that you use the email address for a
distribution list to ensure that our notifications are received and processed quickly.
Step 3: Payment options
Indicate if you want to receive your payments via Direct Deposit o r via US Mail.
F800-065-000 Substitute Statewide Payee and W-902-2016

Step 4: Direct depos it informa tion
Financial ins ti tution name & phone number – enter the name and phone number of the
financial institution where you want your funds deposited. Thismustbe a US institution.
Routing number – this is the 9 digit Bank Identification Number assigned by the American
Banking Association. The routing number is the first 9 numbers at the bottom of your check.
See example on form. Do not use the routing number from a generic deposit slip – thes e be g i n
with the number ‘5.’
Account number – this is your bank account number, and can vary in length. It usually follows
the routing number on the check
Account type – select the kind of account your payment will be deposited into. If you do not
make a selection, funds will be transferred into the checking account.
Authorization Signa ture– in order for us to process the Direct Deposit, we need the
signature of the person on file with the bank.
Ste p 5: W-9
The IRS has issued new regulations governing how we report payments and calculate
withholding. We need thiscomplete, signed W-9 in order to proces s your registration and
verify any ch ang es to it.
1.Legal name of payee – enter the name as it appears on feder al t ax forms.
2.Business name – “doing business as” name. Enter only if different from legal name.
3.Check one box for your IRS reporting type – you must check ONLY one box to indicate if
you are an individual, corporation, non-profit organization,etc.
4.Check if the business is medical or legal - If you are a corporation, S-corporation,
partnership or LLC, and your business is medical or legal, you must check the appropriate box.
See the W-9 instructions for more information about reporting types.
5.Select if you are exempt from backup withholding.
6.Address – enter the PO Box or street addresswhere you would like your 1099 mailed.
7.City, State and ZIP
8.Taxpayer Identification Number – enter the Employer Identification Number (EIN)OR
Social Security Number (SSN) you use with the IRS for the legal name entered. DO NOT
ENTER BOTH. Enter ONLY the one that you use with the IRS for the legal name.
9.SIGN the W-9
Step 6 : Submit to one of the following:
Provider Network Applic ation (WPA)
FAX:360-902-4563
Non-Network Provider Application
FAX:360-902-4484
Crime Victims Compensation
FAX:360-902-5333
Or mail application to: Provider Credentialing & Compliance
PO Box 44261
Oly mpia, WA 9850 4-4261
For questions, contact Provider Credentialing at 360-902-5140 and select option 4.
F800-065-000 Substitute Statewide Payee and W-902-2016


