
Fillable Printable Ia Superintendent Application For Certification 092014
Fillable Printable Ia Superintendent Application For Certification 092014
Ia Superintendent Application For Certification 092014
OhioDepartmentofDevelopmentalDisabilities
County Board Certification Application
(EffectiveSeptember2014)
Instructions:(Please,readcarefully.)
1.Completeaseparateapplicationforeachcertificationrequested.Failuretothoroughlycompleteapplicationforand/orsubmit
requiredsupportingdocumentswillresultinreturnoftheapplicationtotheapplicantbyemail.
2.SubmittheapplicationtotheOhioDepartmentofDevelopmentalDisabilities(DODD),Attn:ProviderCertificationUnitbyemail
toProvider.Ce
[email protected].Emailispreferable,butyoumayalsofaxto614‐728‐7836
.Submitcopiesof
correspondingofficialtranscripts,gradereports,verificationsofseminarcompletion,andverificationofcontinuingprofessional
development.
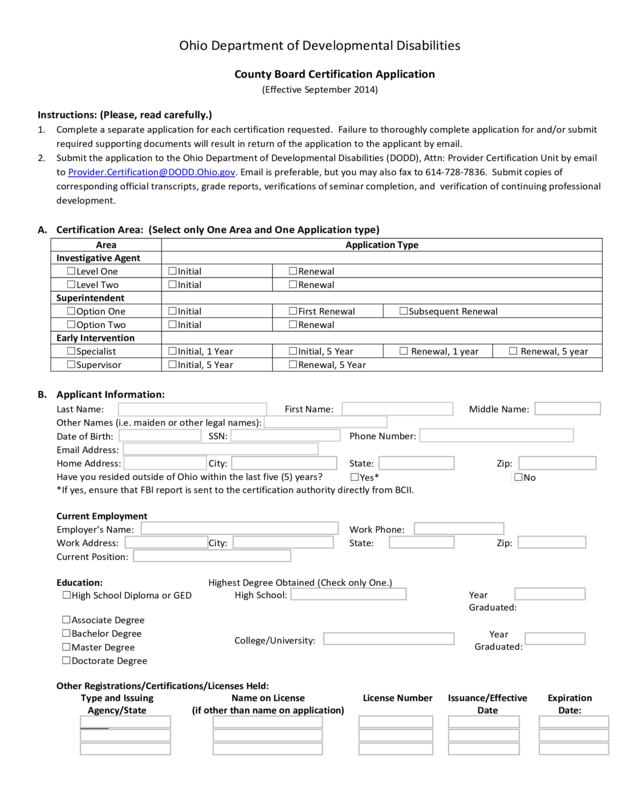
A.CertificationArea:(SelectonlyOneAreaandOneApplicationtype)
AreaApplicationType
InvestigativeAgent
☐LevelOne☐Initial☐Renewal
☐LevelTwo☐Initial☐Renewal
Superintendent
☐OptionOne☐Initial☐FirstRenewal☐SubsequentRenewal
☐OptionTwo☐Initial☐Renewal
EarlyIntervention
☐Specialist☐Initial,1Year☐Initial,5Year☐Renewal,1year☐Renewal,5year
☐Supervisor☐Initial,5Year☐Renewal,5Year
B.ApplicantInformation:
LastName:
FirstName:
MiddleName:
OtherNames(i.e.maidenorotherlegalnames):
DateofBirth:
SSN:
PhoneNumber:
EmailAddress:
HomeAddress:
City:
State:
Zip:
HaveyouresidedoutsideofOhiowithinthelastfive(5)years?
☐Yes*☐No
*Ifyes,ensurethatFBIreportissenttothecertificationauthoritydirectlyfromBCII.
CurrentEmployment
Employer’sName:
WorkPhone:
WorkAddress:
City:
State:
Zip:
CurrentPosition:
Education:HighestDegreeObtained(C
heckonlyOne.)
☐HighSchoolDiplomaorGED
HighSchool:
Year
Graduated:
☐AssociateDegree
College/University:
Year
Graduated:
☐BachelorDegree
☐MasterDegree
☐DoctorateDegree
OtherR
egistrations/Certifications/LicensesHeld:
TypeandIssuing
Agency/State
NameonLicense
(ifotherthannameonapplication)
LicenseNumberIssuance/Effective
Date
Expiration
Date:
C.Convictions/AdverseActions:
Haveyoueverbeenconvictedofanyfelonyormisdemeanor(otherthanaminortrafficoffense)?
Youmustanswerthisquestioneveniftherecordofyourconviction(s)hasbeensealedorexpungedbyacourtoflawand
regardlessofwhetherornottheconvictionappearsonacriminalbackgroundcheck.Ifyouanswer“Yes”,useaseparatesheet
ofpapertoprovideadetailedpersonalaccountofthenatureofth
eoffenseincludingthenameoftheconviction,thedate,the
location(i.e.city,county,andstate),andanexplanationleadingtotheconviction.Iftheconvictionhasbeensealedor
expunged,alsoprovidedetailedinformationregardingthesealingorexpungementandattachacopyofthecourtjournalentry.
☐Yes*☐No
Haveyoueverhadaregistration,certifi c ation,orlicense(excludingaDriver’sLicense)suspendedorrevoked?
(If
youanswer,“Yes”,useaseparatesheetofpapertoexplain.Includeinformationregardingtheparticular
registration/certification/licenseincludingissuingauthority.)
☐Yes☐No
*AnyBCIIand/orFBIreportsmustbesentdirectlyfromBCIIinLondon,OhiotoDODD.
D.RequiredNotice:
Iftheholderoforapplicantforcertificationand/ortheemployingCountyBoardofDDorCouncilofGovernmentbecomes
awarethattheholderoforapplicantforregistrationisguiltyofseriousintemperate,immoral,orconductunbecomingto
his/herposition,and/orisguiltyofseriousincompetenceornegligencewithinthescopeofher/hisduties,and/orhasbeen
arrested,convi
cted,orpledguiltytoanyofthefelonyormisdemeanoroffensesdescribedinAR5123:2‐2‐02,he/sheshallnotify
thecertifyingauthorityinwritingwithin72hours.
E.Applicant’sStatement:
Iherebyattest(certify)thattheinformationcontainedonthisapplicationistruetothebestofmyknowledge.Iagreeto
completethenecessaryseminars,collegecourses,and/orcontinuingprofessionaldevelopmentunitsrequiredtoreceiveinitial
certificationortorenewanexistingcertification.
SignatureofApplicantDateSigned
ReviewerOnly:
SignaturebytheDODDCertificationSpecialistisrequiredforissuanceofcertificationforSuperintendent,Early
InterventionorInvestigativeAgent.
☐Applicanthasmettherequirementsofapplicablewor kexperienceforthecertificationrequested.
☐ApplicanthassuccessfullycompletedtherequiredOr ientationProgram.
☐Applicanthasme
ttherequirementsofapplicableeducation/trainingforth
ecertificationrequested.
Iftheapplicantanswered“Yes”tothefirstquestionunderC,thereviewermustcheckoneofthefollowingboxes:
☐ApplicanthascompletedaBCIIcriminalbackgroundcheckanddoesNOThaveacriminalrecordthatprecludes
issuanceofcertification.
☐Appli
canthascompletedaBCII
criminalbackgroundcheckandhasmettherehabilitationstandards.
SignatureofCertificationAuthorityDateSigned


