
Fillable Printable OPM Form 71
Fillable Printable OPM Form 71
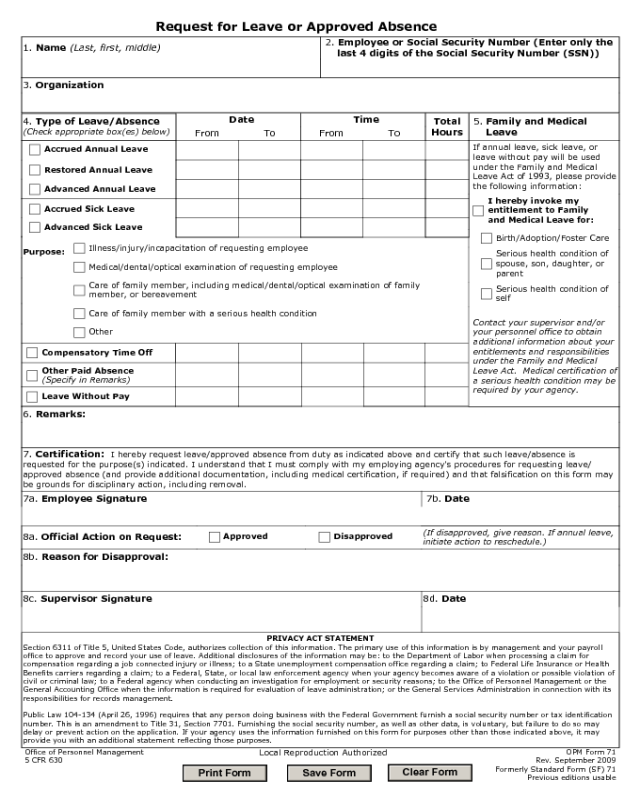
OPM Form 71
Request for Leave or Approved Absence
1. Name (Last, first, middle)
2. Employee or Social Security Number (Enter only the
last 4 digits of the Social Security Number (SSN))
3. Organization
4. Type of Leave/Absence
(Check appropriate box(es) below)
Date
From To
Accrued Annual Leave
Time
From To
Total
Hours
5. Family and Medical
Leave
If annual leave, sick leave, or
leave without pay will be used
under the Family and Medical
Leave Act of 1993, please provide
the following information:
Contact your supervisor and/or
your personnel office to obtain
additional information about your
entitlements and responsibilities
under the Family and Medical
Leave Act. Medical certification of
a serious health condition may be
required by your agency.
I hereby invoke my
entitlement to Family
and Medical Leave for:
Restored Annual Leave
Advanced Annual Leave
Accrued Sick Leave
Advanced Sick Leave
Birth/Adoption/Foster Care
Serious health condition of
spouse, son, daughter, or
parent
Serious health condition of
self
Purpose:
Illness/injury/incapacitation of requesting employee
Medical/dental/optical examination of requesting employee
Care of family member, including medical/dental/optical examination of family
member, or bereavement
Care of family member with a serious health condition
Other
Compensatory Time Off
Other Paid Absence
(Specify in Remarks)
Leave Without Pay
6. Remarks:
7. Certification: I hereby request leave/approved absence from duty as indicated above and certify that such leave/absence is
requested for the purpose(s) indicated. I understand that I must comply with my employing agency's procedures for requesting leave/
approved absence (and provide additional documentation, including medical certification, if required) and that falsification on this form may
be grounds for disciplinary action, including removal.
7a. Employee Signature 7b. Date
8a. Official Action on Request:
(If disapproved, give reason. If annual leave,
initiate action to reschedule.)
8b. Reason for Disapproval:
8c. Supervisor Signature 8d. Date
PRIVACY ACT STATEMENT
Section 6311 of Title 5, United States Code, authorizes collection of this information. The primary use of this information is by management and your payroll
office to approve and record your use of leave. Additional disclosures of the information may be: to the Department of Labor when processing a claim for
compensation regarding a job connected injury or illness; to a State unemployment compensation office regarding a claim; to Federal Life Insurance or Health
Benefits carriers regarding a claim; to a Federal, State, or local law enforcement agency when your agency becomes aware of a violation or possible violation of
civil or criminal law; to a Federal agency when conducting an investigation for employment or security reasons; to the Office of Personnel Management or the
General Accounting Office when the information is required for evaluation of leave administration; or the General Services Administration in connection with its
responsibilities for records management.
Public Law 104-134 (April 26, 1996) requires that any person doing business with the Federal Government furnish a social security number or tax identification
number. This is an amendment to Title 31, Section 7701. Furnishing the social security number, as well as other data, is voluntary, but failure to do so may
delay or prevent action on the application. If your agency uses the information furnished on this form for purposes other than those indicated above, it may
provide you with an additional statement reflecting those purposes.
Approved Disapproved
OPM Form 71
Rev. September 2009
Formerly Standard Form (SF) 71
Previous editions usable
Local Reproduction Authorized
Office of Personnel Management
5 CFR 630
Clear Form
Print Form
Save Form


