
Fillable Printable Return to Work Release Form - The University of Texas at Austin
Fillable Printable Return to Work Release Form - The University of Texas at Austin
Return to Work Release Form - The University of Texas at Austin
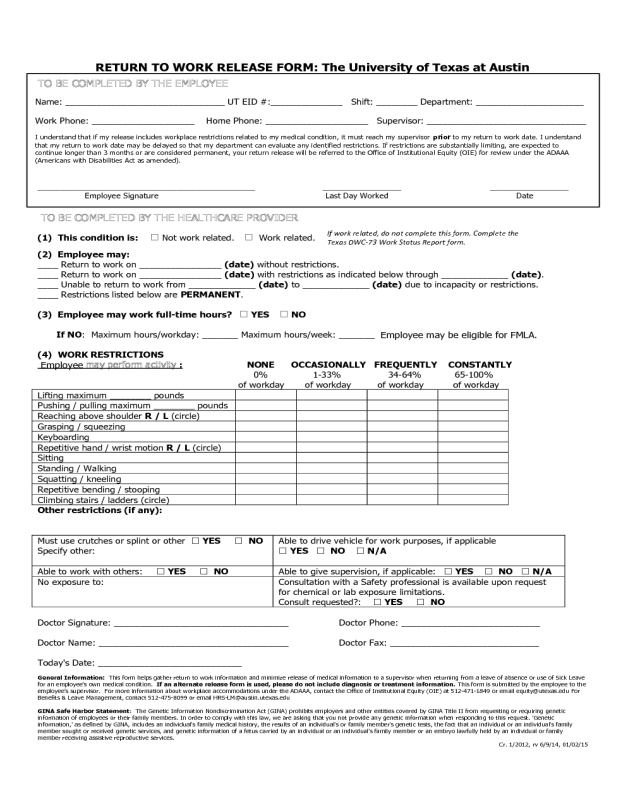
RETURN TO WORK RELEASE FORM: The University of Texas at Austin
TO BE COMPLETED BY THE HEALTHCARE PROVIDER
(1) This condition is: Not work related. Work related.
(2) Employee may:
____ Return to work on ________________ (date) without restrictions.
____ Return to work on ________________ (date) with restrictions as indicated below through _____________ (date).
____ Unable to return to work from _____________ (date) to _____________ (date) due to incapacity or restrictions.
____ Restrictions listed below are PERMANENT.
(3) Employee may work full-time hours?
YES
NO
If NO: Maximum hours/workday: _______ Maximum hours/week: _______
Employee may be eligible for FMLA.
(4) WORK RESTRICTIONS
Employee may perform activity
:
NONE OCCASIONALLY FREQUENTLY CONSTANTLY
0%
1-33%
34-64% 65-100%
of workday of workday of workday of workday
Lifting maximum ________ pounds
Pushing / pulling maximum ________ pounds
Reaching above shoulder R / L (circle)
Grasping / squeezing
Keyboarding
Repetitive hand / wrist motion R / L (circle)
Sitting
Standing / Walking
Squatting / kneeling
Repetitive bending / stooping
Climbing stairs / ladders (circle)
Other restrictions (if any):
Must use crutches or splint or other
YES
NO
Specify other:
Able to drive vehicle for work purposes, if applicable
YES
NO
N/A
Able to work with others:
YES
NO Able to give supervision, if applicable:
YES
NO
N/A
No exposure to:
Consultation with a Safety professional is available upon request
for chemical or lab exposure limitations.
Consult requested?:
YES
NO
Doctor Signature: __________________________________ Doctor Phone: ___________________________
Doctor Name: _____________________________________ Doctor Fax: _____________________________
Today's Date: ____________________________
General Information: This form helps gather return to work information and minimize release of medical information to a supervisor when returning from a leave of absence or use of Sick Leave
for an employee’s own medical condition. If an alternate release form is used, please do not include diagnosis or treatment information. This form is submitted by the employee to the
employee’s supervisor. For more information about workplace accommodations under the ADAAA, contact the Office of Institutional Equity (OIE) at 512-471-1849 or email equity@utexas.edu For
Benefits & Leave Management, contact 512-475-8099 or email [email protected]s.edu
GINA Safe Harbor Statement: The Genetic Information Nondiscrimination Act (GINA) prohibits employers and other entities covered by GINA Title II from requesting or requiring genetic
information of employees or their family members. In order to comply with this law, we are asking that you not provide any genetic information when responding to this request. 'Genetic
information,' as defined by GINA, includes an individual's family medical history, the results of an individual's or family member's genetic tests, the fact that an individual or an individual's family
member sought or received genetic services, and genetic information of a fetus carried by an individual or an individual's family member or an embryo lawfully held by an individual or family
member receiving assistive reproductive services.
Cr. 1/2012, rv 6/9/14, 01/02/15
TO BE COMPLETED BY THE EMPLOYEE
Name: _______________________________ UT EID #:______________ Shift: ________ Department: _____________________
Work Phone: ____________________ Home Phone: ____________________ Supervisor: _______________________________
I understand that if my release includes workplace restrictions related to my medical condition, it must reach my supervisor prior to my return to work date. I understand
that my return to work date may be delayed so that my department can evaluate any identified restrictions. If restrictions are substantially limiting, are expected to
continue longer than 3 months or are considered permanent, your return release will be referred to the Office of Institutional Equity (OIE) for review under the ADAAA
(Americans with Disabilities Act as amended).
_______________________________________________ _________________ _________________
Employee Signature Last Day Worked Date
If work related, do not complete this form. Complete the
Texas DWC-73 Work Status Report form.


