
Fillable Printable Rhode Island Personal Move-in/Move-out Checklist
Fillable Printable Rhode Island Personal Move-in/Move-out Checklist
Rhode Island Personal Move-in/Move-out Checklist
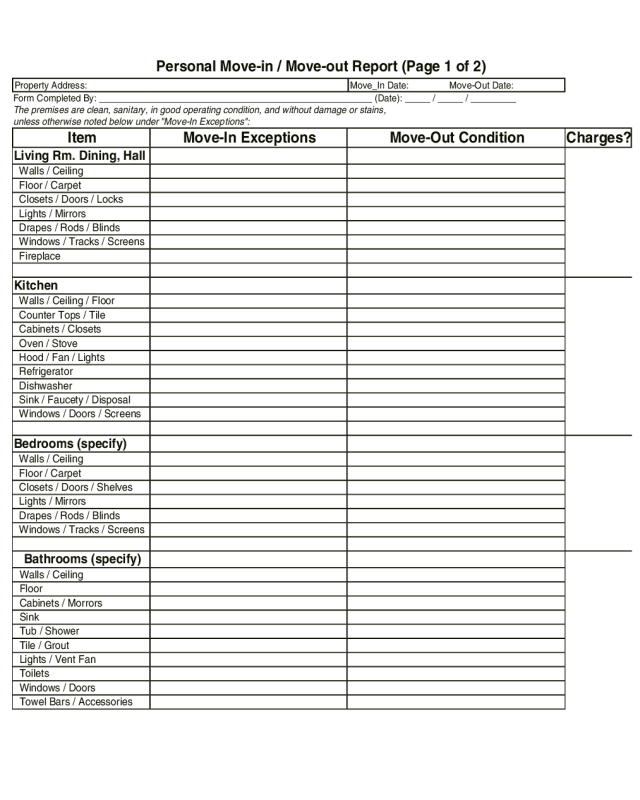
Personal Move-in / Move-out Report (Page 1 of 2)
Property Address:Move_In Date: Move-Out Date:
Form Completed By: ______________________________________________________ (Date): _____ / _____ / _________
The premises are clean, sanitary, in good operating condition, and without damage or stains,
unless otherwise noted below under "Move-In Exceptions":
ItemMove-In ExceptionsMove-Out ConditionCharges?
Living Rm. Dining, Hall
Walls / Ceiling
Floor / Carpet
Closets / Doors / Locks
Lights / Mirrors
Drapes / Rods / Blinds
Windows / Tracks / Screens
Fireplace
Kitchen
Walls / Ceiling / Floor
Counter Tops / Tile
Cabinets / Closets
Oven / Stove
Hood / Fan / Lights
Refrigerator
Dishwasher
Sink / Faucety / Disposal
Windows / Doors / Screens
Bedrooms (specify)
Walls / Ceiling
Floor / Carpet
Closets / Doors / Shelves
Lights / Mirrors
Drapes / Rods / Blinds
Windows / Tracks / Screens
Bathrooms (specify)
Walls / Ceiling
Floor
Cabinets / Morrors
Sink
Tub / Shower
Tile / Grout
Lights / Vent Fan
Toilets
Windows / Doors
Towel Bars / Accessories
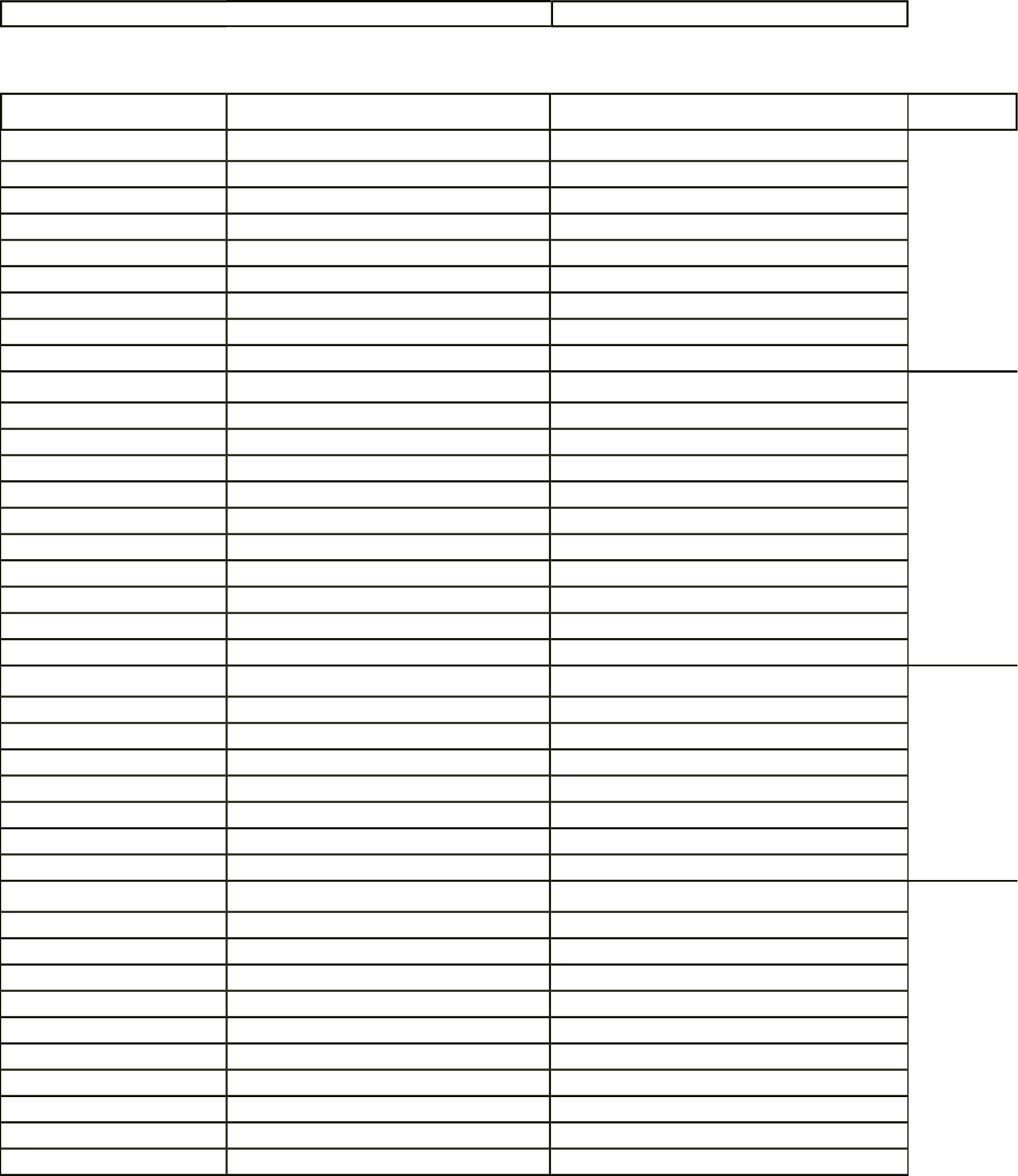
Personal Move-in / Move-out Report (Page 2 of 2)
ItemMove-In ExceptionsMove-Out ConditionCharges?
Washer / Dryer
Heat / AC
Balcony / Deck / Patio
Storage / Parking Area
Garden / Plants / Grass
Smoke Detector
Number of Keys
____Unit ____Entry ____Mailbox ___Other____Unit ____Entry ____Mailbox ____Other
Further Move-In Comments:Move-Out Comments
Date of Move-In Inspection:Date of Move-Out Inspection:
Note Charges / Deposits Here (Indicate dates of payments / charges)
Security Depost:___________ First Month:___________ Last Month:___________Other (Rental):___________ TOTAL:___________
Note Other Move-In Expenses / Deposits, such as keys, locks, etc., if applicable:
TOTAL:___________
Note any refundable / deductable expenses, such as, painting or replacements for which the landlord may be responsible:
TOTAL:___________


