
Fillable Printable SF 1153
Fillable Printable SF 1153
SF 1153
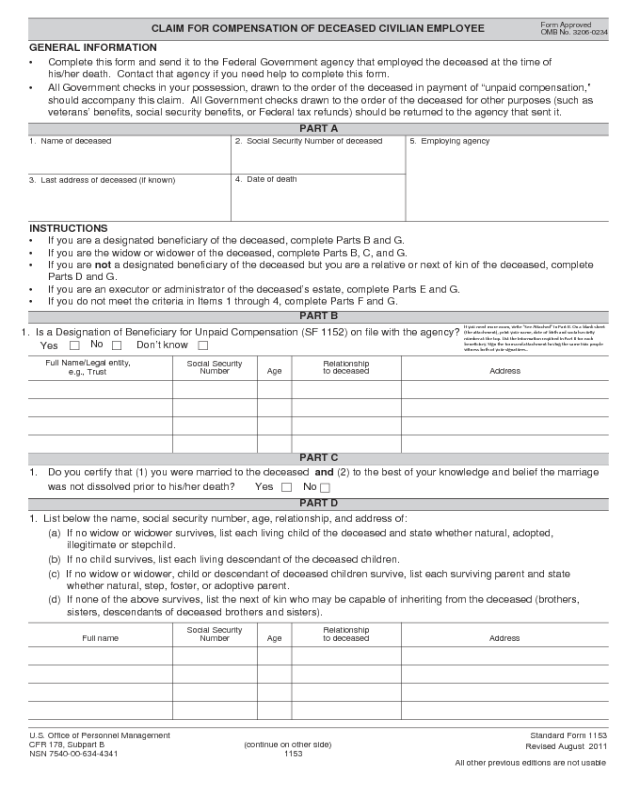
CLAIM FOR COMPENSATION OF DECEASED CIVILIAN EMPLOYEE
Standard Form 1153
Revised August 2011
All other previous editions are not usable
Form Approved
OMB No. 3206-0234
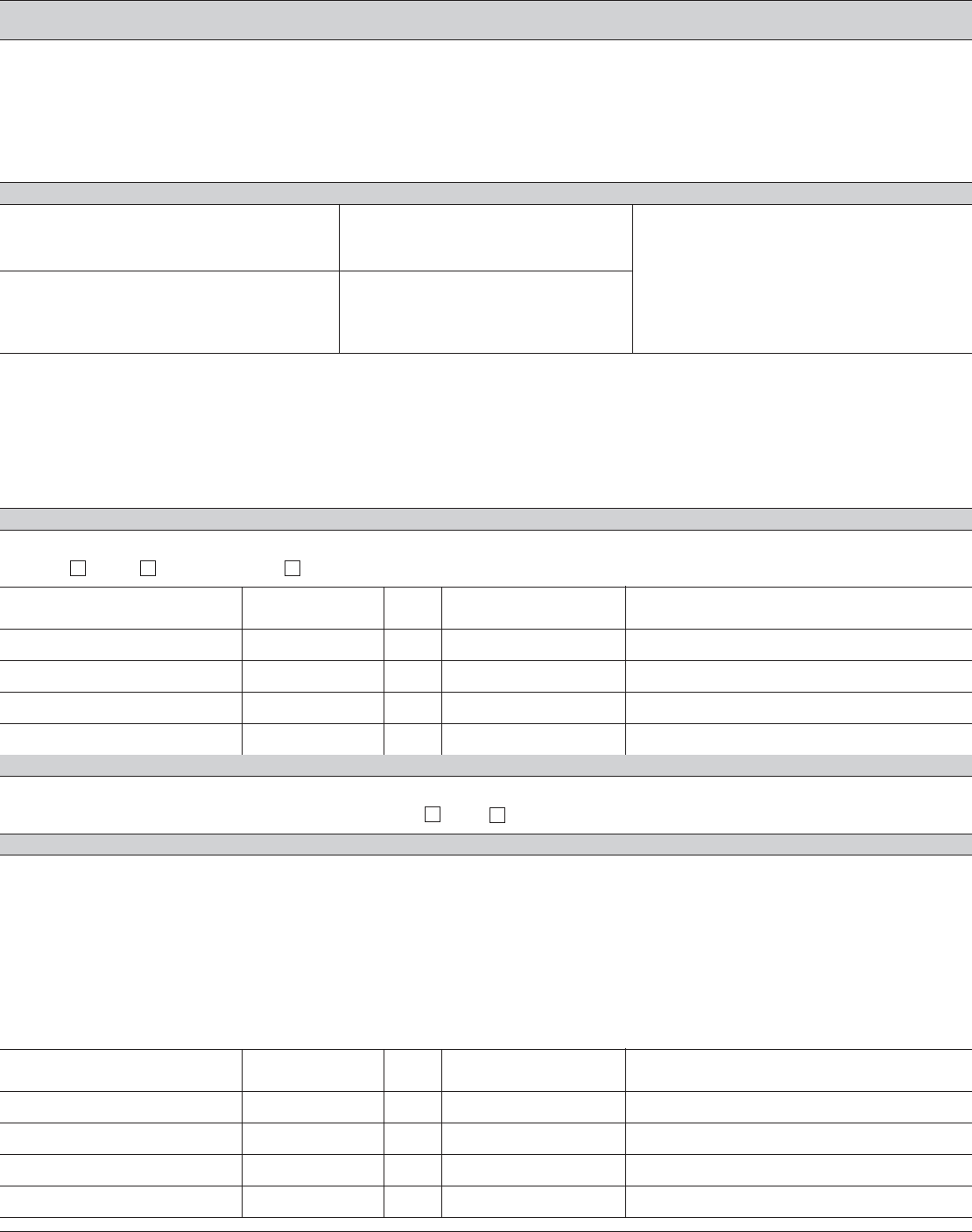
If you need more room, write "See Attached" in Part B. On a blank sheet
(the attachment), print your name, date of birth and social security
number at the top. List the information required in Part B for each
beneficiary. Sign the form and attachment having the same two people
witness both of your signatures..
GENERAL INFORMATION
• Complete this form and send it to the Federal Government agency that employed the deceased at the time of
his/her death. Contact that agency if you need help to complete this form.
• All Government checks in your possession, drawn to the order of the deceased in payment of “unpaid compensation,”
should accompany this claim. All Government checks drawn to the order of the deceased for other purposes (such as
veterans’ benefits, social security benefits, or Federal tax refunds) should be returned to the agency that sent it.
PART A
1. Name of deceased 2. Social Security Number of deceased
3. Last address of deceased (if known)
4. Date of death
5. Employing agency
INSTRUCTIONS
• If you are a designated beneficiary of the deceased, complete Parts B and G.
• If you are the widow or widower of the deceased, complete Parts B, C, and G.
• If you are
not
a designated beneficiary of the deceased but you are a relative or next of kin of the deceased, complete
Parts D and G.
• If you are an executor or administrator of the deceased’s estate, complete Parts E and G.
• If you do not meet the criteria in Items 1 through 4, complete Parts F and G.
PART B
1. Is a Designation of Beneficiary for Unpaid Compensation (SF 1152) on file with the agency?
Yes
No
Don’t know
Full Name/Legal entity,
e.g., Trust
Social Security
Number Age
Relationship
to deceased Address
PART C
1.
Do you certify that (1) you were married to the deceased
and
(2) to the best of your knowledge and belief the marriage
was not dissolved prior to his/her death?
Yes No
PART D
1. List below the name, social security number, age, relationship, and address of:
(a) If no widow or widower survives, list each living child of the deceased and state whether natural, adopted,
illegitimate or stepchild.
(b) If no child survives, list each living descendant of the deceased children.
(c) If no widow or widower, child or descendant of deceased children survive, list each surviving parent and state
whether natural, step, foster, or adoptive parent.
(d) If none of the above survives, list the next of kin who may be capable of inheriting from the deceased (brothers,
sisters, descendants of deceased brothers and sisters).
Full name
Social Security
Number Age
Relationship
to deceased Address
U.S. Office of Personnel Management
CFR 178, Subpart B
(continue on other side)
NSN 7540-00-634-4341
1153
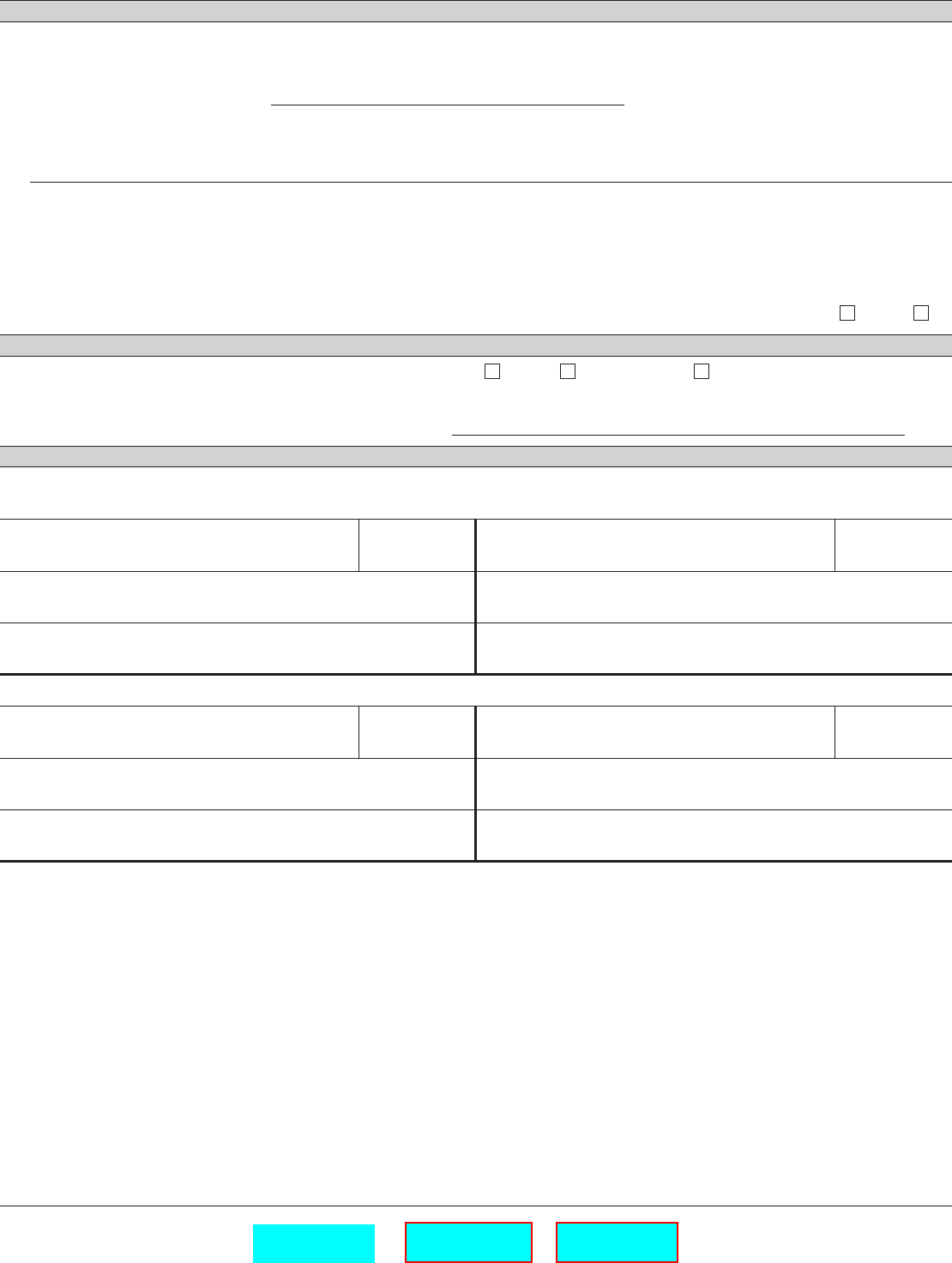
PART E
1. If none of the individuals listed in Parts B and D survives and an executor or administrator of the deceased’s estate has
been appointed, the following statement should be completed.
I/we have been duly appointed
(Executor or Administrator)
of the estate of the deceased, as
evidenced by certificate of appointment herewith, administration having been taken out in the interest of
(Name, address, and relationship of interested relative or creditor)
and such appointment is still in full force and effect.
NOTE:
If making claim as the executor or administrator of the estate of the deceased, no witnesses are required, but a
court certificate evidencing your appointment must be submitted.
2. If no administrator or executor of the deceased’s estate has been appointed, will one be appointed? Yes No
PART F
1. Have funeral expenses of the deceased been paid? Yes No Don’t know
(If paid, receipted bill of the funeral director must be attached.)
Whose money was used to pay the funeral expenses? .
PART G
Fines
,
Penalties
and
Forfeitures
are imposed by law for making false or fraudulent claims against the United States or
making false statements in connection therewith.
Signature of claimant Date
Street address
City, State, and Zip Code
Signature of claimant Date
Street address
City, State, and Zip Code
Two Witnesses are Required
Signature of witness Date
Street address
City, State, and Zip Code
Signature of witness Date
Street address
City, State, and Zip Code
Privacy Act and Public Burden Statement
Solicitation of this information is authorized by the Code of Federal Regulations, Part 178, Subpart B. The information you
furnish will be used to determine the amount, validity, and the person(s) entitled to the unpaid compensation of a deceased
Federal employee. The information may be shared and is subject to verification, via paper, electronic media, or through the use
of computer matching programs to obtain information necessary for determination of entitlement under this program or to report
income for tax purposes. It may also be shared and verified, as noted above, with law enforcement agencies when they are
investigating a violation or potential violation of the civil or criminal law. Public Law 104-134 (April 26, 1996) requires that any
person doing business with the Federal government furnish a Social Security Number or tax identification number. This is an
amendment to title 31, Section 7701. Failure to furnish the requested information may delay or make it impossible for us to
determine your eligibility to receive payments.
We think this form takes an average of 15 minutes per response to complete, including the time for reviewing instructions, getting
the needed data, and reviewing the completed form. Send comments regarding our estimate or any other aspect of SF 1153,
including suggestions for reducing completion time, to the Office of Personnel Management (OPM), Reports and Forms Officer,
Paperwork Reduction (3206-0234), Washington, D.C. 20415-7900. The OMB number 3206-0234 is currently valid. OPM may
not collect this information, and you are not required to respond, unless this number is displayed.
U.S. Office of Personnel Management Standard Form 1153
CFR 178, Subpart B Revised
Aug
2011
Print Form
Save Form
Clear Form


