
Fillable Printable SF 2817
Fillable Printable SF 2817
SF 2817
Federal Employees'
Group Life Insurance
Form Approved:
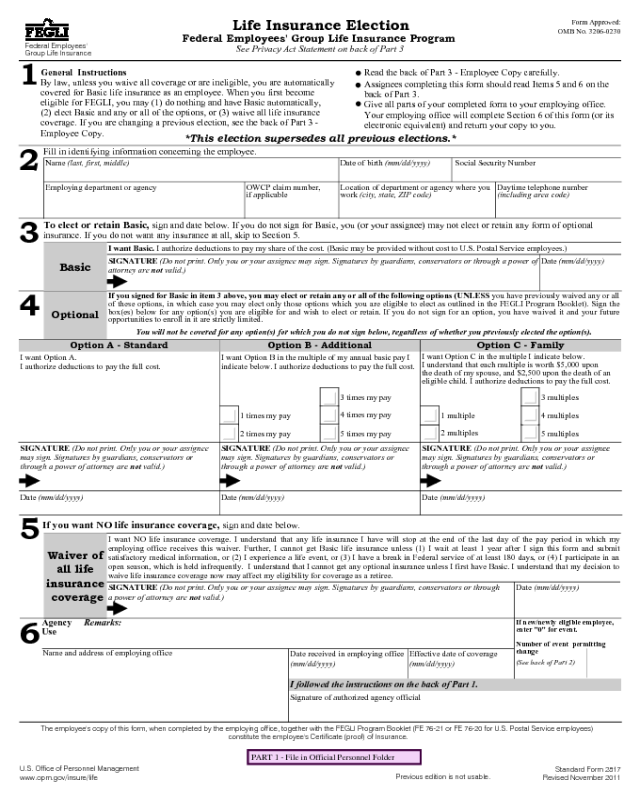
Life Insurance Election
OMB No. 3206-0230
Federal Employees' Group Life Insurance Program
See Privacy Act Statement on back of Part 3
1
General Instructions
.
Read the back of Part 3 - Employee Copy carefully.
By law, unless you waive all coverage or are ineligible, you are automatically
.
Assignees completing this form should read Items 5 and 6 on the
covered for Basic life insurance as an employee. When you first become
back of Part 3.
eligible for FEGLI, you may (1) do nothing and have Basic automatically,
.
Give all parts of your completed form to your employing office.
(2) elect Basic and any or all of the options, or (3) waive all life insurance
Your employing office will complete Section 6 of this form (or its
coverage. If you are changing a previous election, see the back of Part 3 -
electronic equivalent) and return your copy to you.
Employee Copy.
*This election supersedes all previous elections.*
2
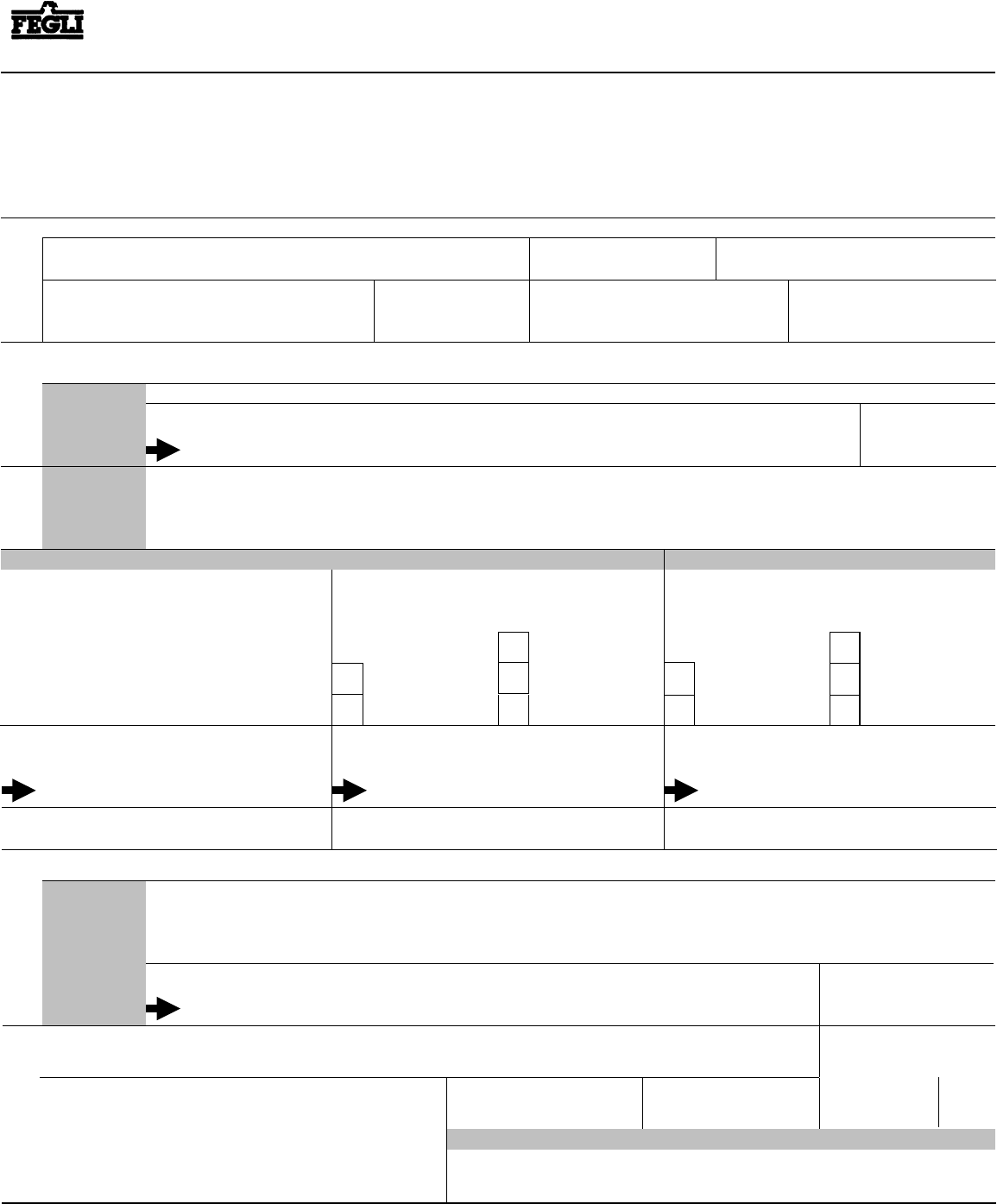
Fill in identifying information concerning the employee.
Name (last, first, middle)
Date of birth (mm/dd/yyyy) Social Security Number
Employing department or agency OWCP claim number,
if applicable
Location of department or agency where you
work (city, state, ZIP code)
Daytime telephone number
(including area code)
Optional
3
SIGNATURE (Do not print. Only you or your assignee may sign. Signatures by guardians, conservators or through a power of
attorney are not valid.)
SIGNATURE (Do not print. Only you or your assignee
may sign. Signatures by guardians, conservators or
through a power of attorney are not valid.)
Option C - FamilyOption B - Additional
I want Basic. I authorize deductions to pay my share of the cost. (Basic may be provided without cost to U.S. Postal Service employees.)
If you signed for Basic in item 3 above, you may elect or retain any or all of the following options (UNLESS you have previously waived any or all
of these options, in which case you may elect only those options which you are eligible to elect as outlined in the FEGLI Program Booklet). Sign the
box(es) below for any option(s) you are eligible for and wish to elect or retain. If you do not sign for an option, you have waived it and your future
opportunities to enroll in it are strictly limited.
To elect or retain Basic, sign and date below. If you do not sign for Basic, you (or your assignee) may not elect or retain any form of optional
insurance. If you do not want any insurance at all, skip to Section 5.
4
I want Option A.
I authorize deductions to pay the full cost.
I want Option B in the multiple of my annual basic pay I
indicate below. I authorize deductions to pay the full cost.
I want Option C in the multiple I indicate below.
I understand that each multiple is worth $5,000 upon
the death of my spouse, and $2,500 upon the death of an
eligible child. I authorize deductions to pay the full cost.
5
If you want NO life insurance coverage, sign and date below.
Date (mm/dd/yyyy)
1 multiple
3 multiples
2 multiples
4 multiples
5 multiples
1 times my pay
3 times my pay
2 times my pay
4 times my pay
5 times my pay
Date (mm/dd/yyyy)
Basic
SIGNATURE (Do not print. Only you or your assignee
may sign. Signatures by guardians, conservators or
through a power of attorney are not valid.)
SIGNATURE (Do not print. Only you or your assignee
may sign. Signatures by guardians, conservators or
through a power of attorney are not valid.)
Date (mm/dd/yyyy) Date (mm/dd/yyyy)
You will not be covered for any option(s) for which you do not sign below, regardless of whether you previously elected the opt ion(s).
Option A - Standard
SIGNATURE (Do not print. Only you or your assignee may sign. Signatures by guardians, conservators or through
a power of attorney are not valid.)
Effective date of coverage
(mm/dd/yyyy)
If new/newly eligible employee,
enter "0" for event.
Number of event permitting
change
I want NO life insurance coverage. I understand that any life insurance I have will stop at the end of the last day of the pay period in which my
employing office receives this waiver. Further, I cannot get Basic life insurance unless (1) I wait at least 1 year after I sign this form and submit
satisfactory medical information, or (2) I experience a life event, or (3) I have a break in Federal service of at least 180 days, or (4) I participate in an
open season, which is held infrequently. I understand that I cannot get any optional insurance unless I first have Basic. I understand that my decision to
waive life insurance coverage now may affect my eligibility for coverage as a retiree.
Signature of authorized agency official
6
Agency
Use
(See back of Part 2)
Name and address of employing office
Date received in employing office
(mm/dd/yyyy)
Date (mm/dd/yyyy)
Remarks:
Waiver of
all life
insurance
coverage
I followed the instructions on the back of Part 1.
The employee's copy of this form, when completed by the employing office, together with the FEGLI Program Booklet (FE 76-21 or FE 76-20 for U.S. Postal Service employees)
constitute the employee's Certificate (proof) of Insurance.
U.S. Office of Personnel Management
Standard Form 2817
www.opm.gov/insure/life
Previous edition is not usable.
Revised November 2011
PART 1 - File in Official Personnel Folder
PRINT
SAVE
CLEAR
Instructions for Agencies
1. Who Should File This Form?
Y
New employees eligible for life insurance who want
optional insurance or no insurance. Note: New employees
who want only Basic do not have to file.
Y
Employees appointed to positions that allow life insurance
coverage following service in positions that did not allow
life insurance coverage.
Y
Employees who want to change their life insurance.
Y
Reinstated employees who filed a previous waiver of any
type of life insurance, were separated from service for at
least 180 days, and wish to elect coverage.
Y
Assignees who want to decrease or cancel coverage.
Y
Department of Defense employees designated "emergency
essential" and civilian employees deployed in support of a
contingency operation per Public Law 110-417.
Give a new employee a copy of the FEGLI Program Booklet
(FE 76-21 or FE 76-20 for U.S. Postal Service employees)
when he or she reports for duty and ask the employee to
return the completed SF 2817 as soon as possible (preferably
before the end of the first pay period), but no later than 60
days after his or her appointment.
Employees with prior government service in non-excluded
positions who were separated after March 31, 1981, should
have an SF 2817 on file in their personnel folders, and that
election or waiver of coverage may still be in effect. Do not
accept a new SF 2817 unless the employee has a break in
Federal service of at least 180 days or is eligible to cancel a
previous waiver that has been in effect for at least one
year, or wishes to reduce coverage.
Until you verify an employee's SF 2817 on file, make
deductions based on his or her statement about earlier
insurance coverage. Once coverage is confirmed, make any
necessary adjustments to correct the withholdings.
An employee may at any time file an SF 2817 to waive or
reduce coverage, unless the employee has assigned his/her
insurance coverage. If the employee has assigned the
insurance, only the assignee(s) may waive or reduce the
coverage (except for Option C which cannot be assigned).
2. How Else Can An Employee Elect More Coverage?
Y
Provide Medical Information. An employee may elect
or increase Basic, Option A, or Option B insurance (but
not Option C), if a previously completed SF 2817
waiving coverage has been in effect for more than one
year, by submitting satisfactory evidence of insurability
via a Request for Insurance, SF 2822. If approved, the
employee should make the election on the SF 2817 and
submit to the employing agency. More details are
contained on the SF 2822.
Y
Experience A Qualifying Life Event. An employee may
elect Basic, Option A, Option B and/or Option C within
60 days following a FEGLI qualifying life event. These
events are: marriage, divorce, spouse's death, or the
acquisition of an eligible child.
For Option B and Option C, an employee may elect from
1 to 5 multiples (up to 5 total) based on the life event.
Y
An employee who is already enrolled in Option B and/or
Option C may elect from 1 to 5 multiples (up to 5 total)
within 60 days based on the life event.
3.
What Should You Review After The Employee
Submits This Form?
Review all three parts of the SF 2817 to see that they are
legible and complete. If an employee signs the box for
Option A, Option B, or Option C, he or she must also sign
Section 3, Basic. If the employee uses a downloaded copy,
be sure all parts are completed. Contact the employee if any
part is unclear.
Only the employee may sign this form in Sections 3, 4, or 5,
with one exception (noted below). Signatures by guardians,
conservators, or through a power of attorney are NOT valid.
Exception: If the employee assigned the insurance, only the
assignee(s) may waive or reduce some or all of the
employee's coverage. In that case, the assignee(s) must sign
the form (although the information in Section 2 must refer to
the employee). Please note that assignees cannot increase the
employee's coverage. Only the employee can do that.
The employee is solely responsible for ensuring that the
SF 2817 accurately reflects his or her intentions.
If the employee is electing new coverage, always make sure
that the authorized agency official confirms that the
employee is eligible for the coverage, and that the official
signs the form in Section 6.
4.
When Did You Receive This?
Enter the date the employing office received this form.
5. What Is The Event Permitting The Change?
Enter the number of the event permitting a change, if
applicable. See the Table of Effective Dates on the back of
Part 2 for event numbers.
6. What Is The Effective Date Of The Coverage?
Enter the effective date of coverage. For new and newly
eligible employees: Basic is effective on the first day the
employee is in a pay and duty status; Optional coverage is
effective on the first day the employee is in a pay and duty
status on or after the day the employing office receives the
SF 2817. For changes in elections, see the Table of Effective
Dates on the back of Part 2. If there is more than one
effective date for this election, the 2nd effective date should
be notated in Part 6 under "Remarks."
7. What Do You Do With Parts 1, 2, and 3?
After completion, give Part 3 to the employee. File Part 1
in the employee's personnel folder. Destroy Part 2 after
payroll office use. Part 3, and the FEGLI Program Booklet
(FE 76-21, or FE 76-20 for U.S. Postal Service employees),
serve as the employee's certificate of insurance.
8. Where Can You Find More Information?
Consult the FEGLI Program Booklet (FE 76-21 or FE 76-20
for U.S. Postal Service employees) or the FEGLI Handbook,
which are available on the FEGLI web site at
www.opm.gov/insure/life.
Back of Part 1
Standard Form 2817
Revised November 2011
Form Approved:
Life Insurance Election
OMB No. 3206-0230
Federal Employees' Group Life Insurance Program
Federal Employees'
Group Life Insurance
1
INELIGIBLE
0000
1000
1100
INSURANCE
A0
B0
C0
D0
SF 50
1005
1101
1102
1103
E5
F1
F2
F3
1011
1012
1013
1014
I1
I2
I3
I4
1114
1115
1020
1120
J4
J5
K0
L0
1001 E1
1104 F4
1015 I5
1021 M1
1002 E2
1105 F5
1111 J1
1022 M2
1003 E3
1010 G0
1112 J2
1023 M3
1004 E4
1110 H0
1113 J3
1024 M4
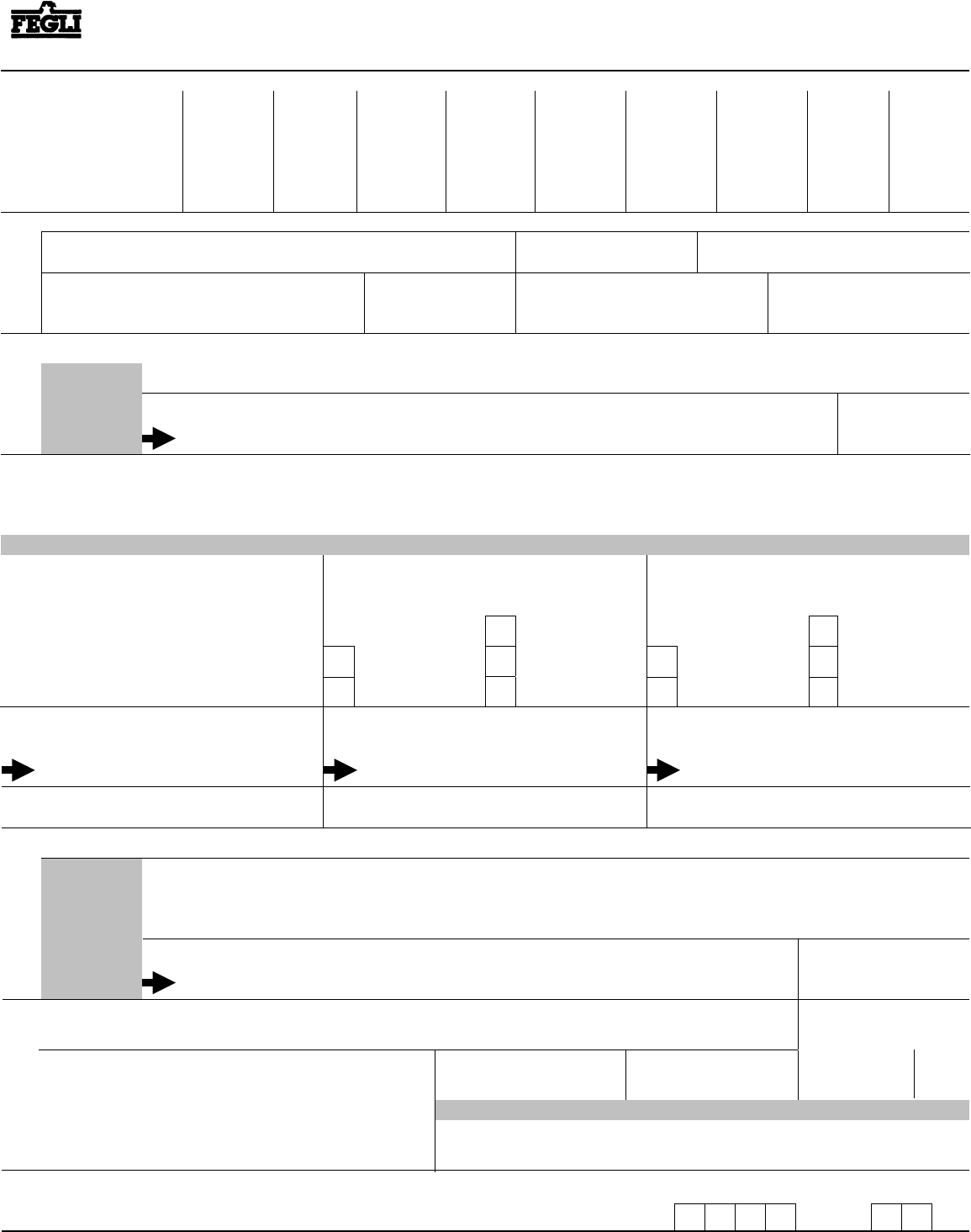
2
Fill in identifying information concerning the employee.
SF 50 Equivalents of Insurance Codes
1025 M5
1031 Q1
1134 R4
1045 U5
1051 Y1
1154 Z4
1121 N1
1032 Q2
1135 R5
1141 V1
1052 Y2
1155 Z5
1122 N2
1033 Q3
1040 S0
1142 V2
1053 Y3
1123 N3
1034 Q4
1140 T0
1143 V3
1054 Y4
1124 N4
1035 Q5
1041 U1
1144 V4
1055 Y5
1125 N5
1131 R1
1042 U2
1145 V5
1151 Z1
1030 90
1132 R2
1043 U3
1050 W0
1152 Z2
1130 P0
1133 R3
1044 U4
1150 X0
1153 Z3
Name (last, first, middle)
Date of birth (mm/dd/yyyy) Social Security Number
Employing department or agency
OWCP claim number,
if applicable
Location of department or agency where you
work (City, state, ZIP Code)
Daytime telephone number
(including area code)
3
SIGNATURE (Do not print. Only you or your assignee may sign. Signatures by guardians, conservators or through a power of
attorney are not valid.)
In item 7: If this block is not signed, enter 0 in ALL FOUR boxes.
If this block is signed, enter 1 in box 1.
4
Date (mm/dd/yyyy)
Basic
In item 7, box 2:
If this block is not signed, enter 0
If this block is signed, enter 1.
Date (mm/dd/yyyy)
1 multiple
3 multiples
2 multiples
4 multiples
5 multiples
1 times my pay
3 times my pay
2 times my pay
4 times my pay
5 times my pay
Date (mm/dd/yyyy) Date (mm/dd/yyyy)
In item 7, box 3:
If this block is not signed, enter 0
If this block is signed, enter the number marked "X"
below.
In item 7, box 4:
If this block is not signed, enter 0
If this block is signed, enter the number marked "X"
below.
5
If you want NO life insurance coverage, sign and date below.
SIGNATURE (Do not print. Only you or your assignee
may sign. Signatures by guardians, conservators or
through a power of attorney are not valid.)
SIGNATURE (Do not print. Only you or your assignee
may sign. Signatures by guardians, conservators or
through a power of attorney are not valid.)
SIGNATURE (Do not print. Only you or your assignee
may sign. Signatures by guardians, conservators or
through a power of attorney are not valid.)
Option C - FamilyOption B - AdditionalOption A - Standard
Waiver of
all life
insurance
coverage
INSTRUCTIONS: Enter codes in the boxes on the right as directed in items 3, 4 and 5 above.
1
Insurance Code
7
SIGNATURE (Do not print. Only you or your assignee may sign. Signatures by guardians, conservators or through a
power of attorney are not valid.)
In item 7: If this block is signed, enter 0 in ALL FOUR boxes.
Date (mm/dd/yyyy)
6
Agency
Use
Name and address of employing office
Remarks:
2 3 4
SF 50
Equivalent
Effective date of coverage
(mm/dd/yyyy)
If new/newly eligible employee,
enter "0" for event.
Number of event permitting
change
(See back of Part 2)
Signature of authorized agency official
I followed the instructions on the back of Part 1.
Date received in employing office
(mm/dd/yyyy)
PART 2 - For Agency Use
U.S. Office of Personnel Management
Standard Form 2817
www.opm.gov/insure/life
Previous edition is not usable.
Revised November 2011

Back of Part 2
Table of Effective Dates: Changes in Life Insurance Coverage
Deductions: Begin, increase, stop or decrease in the same pay period in which coverage begins, increases, stops, or decreases.
Event Allowing Change
Change Permitted? (To elect any option, employee must elect or retain Basic)
Basic Option A - Standard Option B - Additional Option C - Family
1. PROVIDING
MEDICAL
INFORMATION:
Approval of Request for
Insurance (SF 2822) by
the Office of Federal
Employees' Group
Life Insurance (OFEGLI).
Yes. Coverage is automatically effective the first day
the employee is in a pay and duty status on or after
date of OFEGLI's approval.
Time Limit - on or after OFEGLI's date of approval.
If employee is not in a pay and duty status within 60
days, Basic does NOT become effective, and the
employee must start over.
Yes. Coverage is effective the first day the employee is in
a pay and duty status on or after the date of OFEGLI's
approval and the agency receives the SF 2817.
Time Limit - Employee must submit the SF 2817 and be
in a pay and duty status within 60 days after date of
OFEGLI's approval. If employee is not in a pay and duty
status or doesn't submit the SF 2817 within those 60 days,
Option A does not become effective, and the employee
must start over.
Yes. Same as Option A. No. An employee may NOT elect Option C by
providing medical information.
B. Not applicable.
2. LIFE EVENT:
Marriage, divorce, death
of spouse, or acquisition
of an eligible child.
Yes. Coverage is effective the day of the event if the
SF 2817 is received before the event and the
employee is in pay and duty status on the day of the
event. Otherwise, Coverage is effective the first day
in pay and duty status after the event and after
receipt of the SF 2817.
Time Limit - Agency must receive the SF 2817 and
proof of the event within 60 days after the day of the
event.
Yes. Same as Basic.
Coverage - Same as Basic.
Time Limit - Same as Basic.
Yes. Same as Basic.
Employee may elect or increase multiples (up to 5 total).
Coverage - Same as Basic.
Time Limit - Same as Basic.
Yes. Employee may elect or increase multiples (up to 5
total). If the employee has Basic, Coverage is effective
the day the employing office receives the election, or the
date of the event, whichever is later. If Basic and Option
C are elected at the same time, Option C is effective
when Basic becomes effective.
Time Limit - Same as Basic.
(Note: If the employee already has Basic, there is no pay
and duty status requirement for Option C.)
3. REINSTATEMENT:
Employee is reinstated
after a break in service of
at least 180 days in a
position that is not
excluded from life
insurance by law or
regulation.
Yes. Coverage is effective on the first day the
employee is in a pay and duty status, unless waived by
employee.
Yes. Employee may elect Option A within 60 days after
reinstatement. However, if employee does not submit
SF 2817 electing coverage within 60 days after
reinstatement, s/he has the same Optional
insurance carried before the break in service
effective the beginning of the reinstatement.
Same as Option A. Same as Option A.
4. REINSTATEMENT:
Employee is reinstated
after a break in service of
at least 180 days in a
position that is excluded
from life insurance by law
or regulation.
No. However, if employee is later converted to a
non-excluded position, the coverage is effective on the
first day the employee is in a pay and duty status on or
after being converted to such a position.
No. However, if employee is later converted to a
non-excluded position, the coverage is effective on the first
day the employee is in a pay and duty status in the
converted position on or after the date the agency receives
the SF 2817 electing such coverage.
Time Limit - Employee must submit the SF 2817 within 60
days after conversion to an eligible position.
Same as Option A. Same as Option A.
5A. CANCELING/
WAIVING
COVERAGE:
employee/assignee
A. Yes. If the coverage is canceled in the first pay
period, no premiums are due. Otherwise,
coverage stops at the end of the last day of the
pay period in which the agency receives the
SF 2817, with no 31-day extension of coverage.
Time Limit - None. Employee may cancel
coverage at any time. However, if the insurance
is assigned, only the assignee(s) may cancel
A.Same as Basic. A. Same as Basic. A. Same as Basic.
Option C cannot be assigned.
If Option C is canceled because there no longer are
eligible family members, the effective date is
retroactive to the end of the pay period in which
there no longer are any eligible family members.
The employing agency must refund Option C
premiums retroactive to that effective date.
5B. REDUCING
OPTION B and/or
OPTION C
MULTIPLES:
employee/assignee
B. Not applicable. B.Yes. Employee may at any time reduce the number
of multiples, unless the insurance has been assigned.
In that case, only the assignee(s) may reduce coverage
– the employee may not. This new coverage is
effective at the beginning of the pay period following
the one in which the employing office receives the
SF 2817.
B.Yes. Employee may at any time reduce the number
of multiples. This new coverage is effective at
the beginning of the pay period following the
one in which the employing office receives the
SF 2817. Assignee(s) cannot reduce Option C.
6. Open Season. If permitted under conditions specified by OPM. Same as Basic. Same as Basic. Same as Basic.
or
Standard Form 2817, Revised November 2011
0. New/Newly Eligible
Employee:
Yes. See "Instructions to Agencies", #5, back of
Part 1.
Yes. Same as Basic. Yes. Same as Basic. Yes. Same as Basic.
7. CERTAIN DEPT. OF
DEFENSE AND
CIVILIAN
EMPLOYEES
AFFECTED
BY PUBLIC LAWS
106-398 AND 110-417:
Yes, if employing agency determines employee meets
criteria to elect coverage. Coverage is effective the
first day the employee is in a pay and duty status on or
after the date the agency receives the SF 2817.
Time Limit - Agency must receive the SF 2817
within 60 days of the date the employee receives
official notice of deployment in support of a
contingency operation or designation as an emergency
essential employee.
Same as Basic. Same as Basic.
Employee may elect or increase multiples (up to 5
total).
No. An employee may NOT elect Option C via these
provisions of law.

Back of Part 3
Instructions for Employees
Chapter 87, title 5, U.S. Code, Federal Employees' Group Life Insurance, authorizes solicitation of this information. The data you furnish will be used to determine your life insurance coverage. This
information may be shared and is subject to verification, via paper, electronic media, or through the use of the computer matching programs, with national, state, local or other charitable or social
security administrative agencies to determine and issue benefits under their programs or law enforcement agencies, when they are investigating a violation or potential violation of civil or criminal law.
Executive Order 9397 (November 22, 1943) authorizes use of the Social Security Number to distinguish between the applicant and people with similar names. Failure to furnish the requested
information may result in your agency's inability to determine your life insurance coverage.
We estimate this form takes an average of 15 minutes to complete including the time for getting the needed data and reviewing both the instructions and completed form. Send comments regarding our
estimate or any other aspect of this form, including suggestions for reducing completion time, to the Office of Personnel Management (OPM), Retirement Services Publications Team (3206-0230),
Washington, DC 20415-3430. The OMB Number, 3206-0230 is currently valid. OPM may not collect this information, and you are not required to respond, unless this number is displayed.
Privacy Act and Public Burden Statements
1.
General Information
The major provisions of this program are described in the Federal
Employees' Group Life Insurance (FEGLI) Program Booklet (FE 76-21
or FE 76-20 for U.S. Postal Service employees). Please read the entire booklet
carefully. Your completed copy of this election form (SF 2817) and the
FEGLI Program Booklet constitute your certificate (proof) of insurance.
These publications, as well as comprehensive FEGLI information, are
available at www.opm.gov/insure/life.
Standard Form 2817
Revised November 2011
6. I Am An Assignee. What Can I Do?
If you are completing this form in order to cancel some or all of the
employee's life insurance coverage, you must sign the form. The
information in Section 2 of the form refers to the employee, but you must
sign in Section 3, 4 or 5, as applicable. Indicate "assignee" after your
2.
I Am A New Employee or Newly Eligible for Life Insurance. What
Do I Need To Know?
You are automatically enrolled in Basic (even if you don't complete this form)
unless you waive it. If you waive Basic, you automatically waive all forms of
Optional insurance. You will not have any Optional insurance unless you elect it.
To elect Basic: You do not have to submit this form unless you also wish to
elect Optional insurance.
To waive Basic: Sign Section 5 of the form and give it to your employing
office. Your agency will withhold Basic premiums from your salary from
your first day at work in a pay status UNLESS you submit your waiver before
the end of your first pay period.
To elect Optional: Sign Section 3 and one or more of the blocks in Section 4
of the form and give it to your employing office within 60 days after the date
you are appointed or first become eligible for life insurance.
To waive Optional: If you do not sign for a particular type of Optional
coverage in Section 4, you automatically waive that coverage.
3.
I Am An Employee With Prior Government Service. What Do I
Need To Know?
When you return to work after a break in service of less than 180 days, your
human resources office will automatically enroll you in the same coverage
that you had before you left your prior position, if any. This coverage will be
effective on your first day in a pay and duty status in a FEGLI eligible
position. You will have to qualify to elect other coverage (open season,
providing medical information, or a life event). If you waived some coverage,
then the waiver of that coverage is still in effect.
When you return to work after a break in service of 180 days or more, your
human resources office will automatically enroll you in Basic and the same
Optional insurance that you had in your prior position. This coverage will be
effective on your first day in a pay and duty status in a FEGLI eligible
position. You may elect more insurance (if you don't already have the
maximum) within 60 days of your appointment to an eligible position. If you
previously waived coverage then that waiver is no longer in effect. You will
automatically be enrolled in Basic, unless you file a new waiver.
4.
5.
If you waive your insurance when you return to Federal Service as a
reemployed annuitant, you also waive your insurance with your retirement
annuity. You will have no FEGLI life insurance. It is important that you
contact your human resources office and inform them that you are a
reemployed annuitant. More details can be found in OPM Form 1482,
Agency Certification of Status of Reemployed Annuitants.
See the FEGLI Program Booklet (FE 76-21 or FE 76-20 for U.S. Postal
Service Employees) for more details.
I Am A Reemployed Annuitant. What Do I Need To Know?
What If I Assigned My Coverage?
If you have assigned your insurance by filing an RI 76-10, Assignment of
Federal Employees' Group Life Insurance, you may not cancel any of your
insurance coverage (except Option C). Only the assignee(s) may cancel your
coverage. However, you may elect new coverage if you otherwise meet the
requirements for electing such coverage. Any new coverage you elect will
automatically be subject to your existing assignment, except for Option C,
which you cannot assign. All assignments are automatically canceled after a
break in service of at least 31 days, or upon cancellation of all life insurance
coverage by the assignee(s).
signature. Return the completed form to the employee's employing office. If
the insured is an annuitant, return the completed form to OPM, Retirement
Operations Center, P.O. Box 45, Boyers, PA 16017-0045. See #11 for where
to return the completed form if the insured is a compensationer.
Be Sure You Sign For All Options You Want. This election supersedes all
previous ones. If you have optional coverage and wish to keep it, you must
sign the appropriate box(es). If you do not sign for it, you have waived it.
7.
How Do I Complete The Form?
Follow the instructions for each item carefully. After you fill out the form,
review it to be sure it is complete and correct. The following checklist should
help.
If you sign Section 3, you elect (or retain) Basic.
If you sign any block in Section 4, you elect (or retain) Optional Insurance.
You must also elect (or retain) Basic by signing Section 3.
If you sign Section 4 for Option B and/or Option C, you must also mark
one of the five boxes to show how many multiples you wish to elect (or
retain). Do not mark more than one box.
If you sign Section 5, you waive all FEGLI coverage.
Only you, the employee, may sign this form. Signatures by guardians,
conservators, or through a power of attorney are not acceptable.
Exception: If you have assigned your insurance, only the assignee(s) may
cancel some or all of your coverage. In that case, the assignee(s) must sign
the form (although the information in Section 2 must refer to you).
REMEMBER THAT YOU, NOT YOUR AGENCY, ARE
RESPONSIBLE FOR ENSURING THAT YOUR SF 2817 (OR ITS
ELECTRONIC EQUIVALENT) IS CORRECT AND ACCURATELY
REFLECTS YOUR INTENTIONS. IF YOU DO NOT SIGN FOR IT,
YOU HAVE CANCELED/WAIVED IT.
8.
Open Seasons
If you elected coverage during an Open Season, and that coverage has not yet
become effective, and you want to make a further change to your FEGLI
coverage on this SF 2817, you should check with your employing office.
That office can tell you about any special election procedures that may apply.
9.
What If I Waive or Reduce My Coverage?
If you do not sign for a particular type of coverage, you have waived that
coverage. If you waive Basic or one or more of the options, your opportunities
to enroll in the coverage you waived are strictly limited. A waiver may
also affect your eligibility to continue coverage into retirement. See the
FEGLI Program Booklet (FE 76-21 or FE 76-20 for U.S. Postal Service
employees) for more details.
10.
Where Do I Send The Completed Form?
After you have completed this form and verified that it accurately reflects your
intentions, send the entire form (without separating the parts) to your human
resources office. Do not send the form to OPM or OFEGLI.
11.
What If I Receive Workers' Compensation?
If you are receiving compensation payments from the Office of Workers'
Compensation Programs (OWCP), provide your OWCP number in Section 2
of the form. If you are still employed, return the completed form to your
employing office. If you are not still employed or if you have been receiving
compensation payments for at least 12 months, see your human resources
office about your continued eligibility under the FEGLI Program.
12.
How Do I Verify That My Agency Processed My Election?
After your employing office processes your election form, you will receive
an SF 50, Notification of Personnel Action. A two digit code appearing on
the SF 50 will explain your insurance coverage. These codes are explained
in Part 2 of the SF 2817. Also check your pay statement for the correct
withholdings. If you are insured as a compensationer, you will receive a notice
from OPM which will explain your insurance coverage.
13.
Where Do I Get More Information About The FEGLI Program?
Consult the FEGLI Program Booklet (FE 76-21 or FE 76-20 for U.S. Postal
Service employees) or the FEGLI Handbook (RI 76-26), which are available
on the FEGLI web site at www.opm.gov/insure/life.


