
Fillable Printable Application For Certified Copies - Ohio
Fillable Printable Application For Certified Copies - Ohio
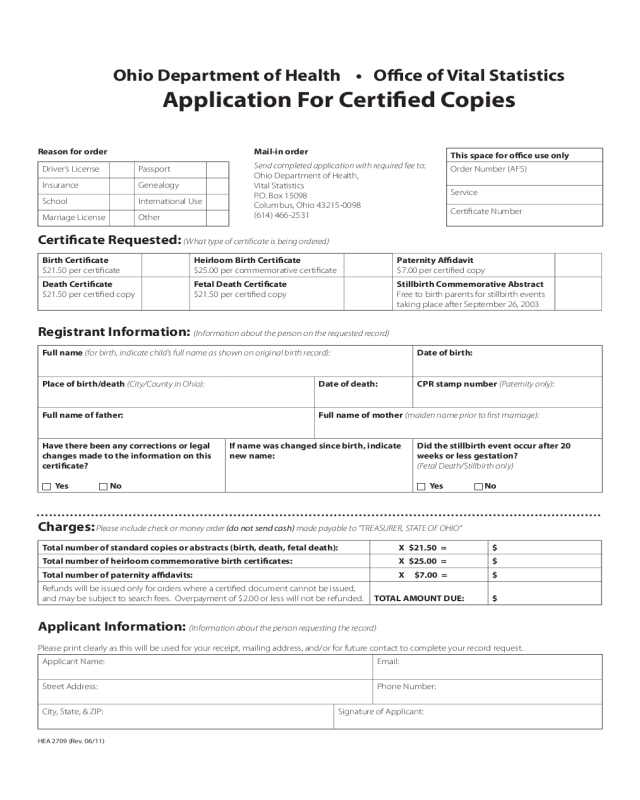
Application For Certified Copies - Ohio
OhioDepartmentofHealth•OceofVitalStatistics
Application For Certied Copies
Reason for order
Driver’s License Passport
Insurance Genealogy
School International Use
Marriage License Other
Mail-in order
Send completed application with required fee to:
Ohio Department of Health,
Vital Statistics
P.O. Box 15098
Columbus, Ohio 43215-0098
(614) 466-2531
This space for oce use only
Order Number (AFS)
Service
Certicate Number
Certicate Requested: (What type of certicate is being ordered)
Birth Certicate
$21.50 per certicate
Heirloom Birth Certicate
$25.00 per commemorative certicate
Paternity Adavit
$7.00 per certied copy
Death Certicate
$21.50 per certied copy
Fetal Death Certicate
$21.50 per certied copy
Stillbirth Commemorative Abstract
Free to birth parents for stillbirth events
taking place after September 26, 2003
Registrant Information: (Information about the person on the requested record)
Full name (for birth, indicate child’s full name as shown on original birth record): Date of birth:
Place of birth/death (City/County in Ohio): Date of death: CPR stamp number (Paternity only):
Full name of father: Full name of mother (maiden name prior to rst marriage):
Have there been any corrections or legal
changes made to the information on this
certicate?
c Yes c No
If name was changed since birth, indicate
new name:
Did the stillbirth event occur after 20
weeks or less gestation?
(Fetal Death/Stillbirth only)
c Yes c No
Charges: Please include check or money order (do not send cash) made payable to “TREASURER, STATE OF OHIO”
Total number of standard copies or abstracts (birth, death, fetal death): X $21.50 = $
Total number of heirloom commemorative birth certicates: X $25.00 = $
Total number of paternity adavits: X $7.00 = $
Refunds will be issued only for orders where a certied document cannot be issued,
and may be subject to search fees. Overpayment of $2.00 or less will not be refunded. TOTAL AMOUNT DUE: $
Applicant Information: (Information about the person requesting the record)
Please print clearly as this will be used for your receipt, mailing address, and/or for future contact to complete your record request.
Applicant Name: Email:
Street Address:
Phone Number:
City, State, & ZIP:
Signature of Applicant:
HEA 2709 (Rev. 06/11)


