
Fillable Printable Basic Memorandum of Understanding Sample
Fillable Printable Basic Memorandum of Understanding Sample
Basic Memorandum of Understanding Sample
Contract # _________
Memorandum of Understanding
Between
{insert name of clinic or health plan}
and
[SPONSOR]
I. Parties of the Memorandum
Parties to this Memorandum of Understanding (Memorandum) are:
A. [SPONSOR], the primary sponsor of the [name of collaborative]. Referred to as the
Collaborative from this point forward.
B. Clinic or health plan address, phone, fax, and e-mail address are as follows:
Manager for {INSERT
HEALH PLAN OR CLINIC}
is:
Manager for [SPONSOR] is:
Contractor Name
Address
City, State Zip Code
Phone: ( )
Fax: ( )
E-mail:
Name
[SPONSOR]
Address
City, State, ZIP
Phone: ( )
Fax: ( )
E-mail:
II. Purpose
The purpose of this memorandum is to specify the agreements of [SPONSOR], and the
{insert health plan or clinic} as participants in the Collaborative. The parties to this
memorandum agree to participate in this health care quality improvement project. The
goal of the project is to improve the quality of [chronic condition] care in a cost-effective
manner through partnerships and collaborations using proven, evidence-based practices.
In addition the health plan or clinic agrees to work to achieve improvements in
[mandatory measures listed here].
This memorandum also specifies the responsibilities of co-sponsors of and organizations
supporting the Collaborative:
[additional sponsor here]
1
Improving Chronic Illness Care is a national program of the Robert Wood Johnson
Foundation located at the MacColl Institute for Healthcare Innovation in the Center
for Health Studies at Group Health Cooperative of Puget Sound.
The participants in the Collaborative will implement the Chronic Care Model using the
rapid cycle change process and breakthrough series methodology developed by the
Institute for Healthcare Improvement and Associates in Process Improvement. Clinics
with or without a health plan partner will develop a population-based approach to
creating patient-centered systems of care. Through three learning sessions, participants
will learn how to apply a variety of change strategies within their health care delivery
system and achieve those changes through quality improvement methodology.
III. Term of the Memorandum
The effective date of this memorandum shall be the date of execution and shall continue
in effect until modified or terminated by either party or until [one month after the final
event].
IV. Clinic Responsibilities
For this Collaborative, a clinic is defined as one or more locations where primary care is
delivered by two or more primary care providers. Multiple locations are administratively
linked together to deliver care as a system.
A. Select a team of at least three people: one representing administration and two
clinicians with an interest in [condition]. For example: MD, RN, RD, RPh, NP, PA.
One of these people will be the day-to-day leader and one will be the primary care
champion.
B. As a team, participate in each of three, two-day learning sessions and the Outcomes
Congress, beginning [insert dates of all sessions].
C. Expenses include travel, lodging, meeting registration of [$ amount] per person per
Learning Session and dedicated staff time to implement changes determined
necessary to reach desired outcomes.
D. Define, with your clinic team, specific outcomes you wish to achieve.
E. Report on the required outcome measures of the Collaborative.
The percent of the pilot [condition] population with:
[mandatory measures]
a documented self-management goal
If the clinic is working with a health plan, these outcomes must be defined
together.
F. The clinic will work to spread the Collaborative throughout its administrative system.
The degree of this spread depends upon the administrative structure of the clinic.
G. Present storyboards illustrating progress at each Learning Session and the Outcomes
Congress.
2
H. Use rapid change cycles to implement the Chronic Care Model and report progress
toward identified outcomes.
I. Submit monthly reports to [SPONSOR or other party] using specific reporting forms,
delineating progress toward identified clinic specific outcomes. (See Attachment A).
If working with a health plan, collaborate on the submission of the monthly report.
J. Participate in the communication network established by [SPONSOR or other party to
MOU] to provide support throughout the collaborative.
K. Report on the achievements of selected outcome measures at the Outcomes Congress
on [date]. If working with a health plan, report outcomes together.
L. Maintain and safeguard the confidentiality of privileged data or information––written,
photographed, electronically recorded or generated and/or acquired by {insert clinic
name}––which can be used to identify an individual patient, practitioner,
participating provider organization, facility, health plan or patient population.
V. Health Plan Responsibilities
All Health Plans must be partnered with a clinic to participate in the Collaborative.
A. Select a team of at least two people representing the suggested categories of
administration, medical director or quality coordinator.
B. Select a clinic partner through which the plan does business to participate in the
Collaborative.
C. Participate in each of three, two-day learning sessions and the two-day Outcomes
Congress beginning [dates here].
D. Health plan expenses will include travel, lodging, [$ amount] registration per person
per Learning Session and dedicated staff support to assist clinic partner.
E. Define, with your clinic partner, the specific outcomes for your health plan/clinic
team.
F. Report on the required outcome measures of the Collaborative.
The percent of the pilot [condition] population with:
[mandatory measures here]
a documented self-management goal
G. Facilitate and provide support for your clinic partner to implement the Chronic
Disease Model to achieve lasting change within the clinic delivery system.
H. Assist in the completion of monthly reports to [SPONSOR or other party to MOU]
identifying progress and rapid change cycles implemented. (See Attachment A).
Assist in the creation of storyboards with clinic partner for presentation at each
Learning Session.
I. Participate in the communication network established by [SPONSOR or other party to
MOU] to provide support throughout the Collaborative.
J. Maintain and safeguard the confidentiality of privileged data or information, written,
photographed, or electronically recorded, generated and/or acquired by {insert health
plan name} which can be used to identify an individual patient, practitioner,
participating provider organization, facility, health plan or patient population.
K. CHANGE IN STATUS - In the event of substantive change in the legal status,
organizational structure, or fiscal reporting responsibility of the Health Plan, the
3
Health plan agrees to notify [SPONSOR] project manager of the change. Health Plan
shall provide notice as soon as practicable, but no later than thirty days after such a
change takes effect.
VI. [SPONSOR] Responsibilities
A. Provide leadership, coordination and partial funding for three, two-day Collaborative
learning sessions and a two-day Outcomes Congress, a reporting structure, data
analysis, marketing and promotion, technical support to teams and communication
methodologies.
B. Document in-kind support provided by all participants in the Collaborative.
C. Sign a Memorandum of Understanding with each participating team, health plan and
supporting organization.
D. Promote participation in the Collaborative and follow-up on all issues related to the
administration of the Collaborative.
E. Provide technical support to teams to implement the Chronic Care Model.
F. Execute a contract with [other party to MOU] to market the Collaborative, enroll
teams, coordinate the delivery of the learning sessions and Outcomes Congress,
review and score the team monthly reports, provide technical assistance to the teams,
maintain a communication system, provide data analysis, and faculty support. [May
be solely completed by sponsor.]
G. Execute a Memorandum of Understanding with the MacColl Institute for Healthcare
Innovation/Group Health Cooperative of Puget Sound to provide faculty and
materials for each Learning Session, technical assistance to project teams, marketing
support, and consultation with the leadership team to coordinate the Collaborative.
H. Promote the process and outcomes of the Collaborative to local, state and national
forums and the media.
I. Conduct regular conference calls with the leadership team to provide oversight to the
project.
J. Assure adherence to internal confidentiality procedures during the course of the
Collaborative. These procedures apply to monthly activity reports, technical
consultation, design of the Collaborative communication system, written reports and
all data or information, written, photographed or electronically recorded, generated
and/or acquired by [SPONSOR] which can be used to identify an individual patient,
practitioner, participating provider organization, facility, health plan or patient
population.
VII. [SPONSOR or other party to MOU] Responsibilities [Note, these may all become part of
section VI if the SPONSOR has not subcontracted these duties.]
Under a contract executed between [SPONSOR] and [SPONSOR or other party to
MOU], [SPONSOR or other party to MOU] will conduct the activities detailed below in
items A through H.
4
A. Register health plan and/or clinic teams for three, two-day Collaborative Learning
Sessions in [dates].
B. Plan and implement each Learning Session and the Outcome Congress including:
Develop the agenda in consultation with [SPONSOR], the Improving Chronic
Illness Care national program and Collaborative faculty
Provide on-site support to facilitate each Learning Session and the Outcomes
Congress
Coordinate all speakers
Assemble all handout materials
Coordinate storyboard set-up
Coordinate on-site arrangements and payment to the facility
C. Facilitate receipt, analysis and scoring of monthly reports from participating teams.
Reports are used to track individual team progress toward required and selected team
measures.
D. Monitor the progress of each team providing consultation to achieve the measures
selected by the team.
E. Maintain a communication system for the participating teams to share resources and
for problem solving.
F. Participate in all leadership team conference calls.
G. At the learning sessions and Outcomes Congress, report the progress toward the
overall outcome measures of the collaborative to improve glycemic blood pressure
and lipid control and self-management support.
H. Assure adherence to internal confidentiality procedures during the course of the
Collaborative. These procedures are needed to prevent identification of an individual
patient, practitioner, participating provider organization, facility, health plan or patient
population. These procedures apply to monthly activity reports, technical
consultation, design of the Collaborative communication system, written reports and
all data or information, written, photographed or electronically recorded, generated
and/or acquired by [SPONSOR or other party to MOU].
VIII. Improving Chronic Illness Care is a national program of the Robert Wood Johnson
Foundation located at the MacColl Institute for Healthcare Innovation in the Center for
Health Studies at Group Health Cooperative of Puget Sound.
As an in-kind supporter to the Collaborative, the MacColl Institute for Healthcare
Innovation agrees to provide the support listed in items A through F.
A. Participate in selected leadership conference calls to provide consultation for the
coordination of the Collaborative.
B. Provide faculty support for three, two-day learning sessions and the two-day
Outcomes Congress. [dates]
C. Provide the Chronic Care Model and templates for the content of learning sessions 1,
2, 3 and the Outcomes Congress that addresses the Chronic Care Model and Rapid
Cycle quality improvement methology as applied to chronic illness care.
5
D. Provide consultation for the development of the agenda for each Learning Session and
the Outcomes Congress.
E. Maintain an active literature review of evidence-based interventions to promote the
implementation of the Chronic Care Model.
F. Maintain and safeguard the confidentiality of privileged data or information–written,
photographed, or electronically recorded, generated and/or acquired by MacColl
Institute of Healthcare Innovation–which can be used to identify an individual patient,
practitioner, participating provider organization, facility, health plan or patient
population.
G. ICIC may take on additional roles, such as analysis and scoring of monthly reports,
participation in monthly telephone calls with teams depending on the expertise of [the
SPONSOR].
IX. Amendment of the Memorandum
This memorandum may be amended at any time by mutual agreement of the parties.
Such amendments shall not be binding upon either party unless they are in writing and
signed by personnel authorized to bind each of the parties.
X. Termination of Memorandum
Either party may terminate this Agreement upon 14 days prior written notification to the
other party. If this agreement is so terminated, the parties shall be liable only for
performance rendered or costs incurred in accordance with the terms of this Agreement
prior to the effective date of termination.
XI. Costs
Unless otherwise specified within the agreement, any and all expenses incurred by the
participants of this collaborative project are the responsibility of the participant.
ENTIRE AGREEMENT
This contract, including referenced exhibits, represents all the terms and conditions agreed upon
by the parties. No other understandings or representations, oral or otherwise, regarding the
subject matter of this contract shall be deemed to exist or to bind any of the parties hereto.
CONFORMANCE
If any provision of this agreement violates any statute or rule of law of the State of [name], it is
considered modified to conform to that statute or rule of law.
APPROVAL
This Memorandum of Understanding shall be subject to the written approval of the
[SPONSOR]'s authorized representative and shall not be binding until so approved. The contract
may be altered, amended, or waived only by a written amendment executed by both parties.
6
THIS MEMORANDUM OF UNDERSTANDING, consisting of seven pages and one
attachment, is executed by the persons signing below who warrant that they have the authority to
execute the Memorandum of Understanding.
____________________________________________ ____________________
Contractor Signature Date
____________________________________________ ____________________
[SPONSOR] Contracting Officer Date
7
Attachment A
Sample Monthly Report for Diabetes Team
Organization: Rocky Road Clinic
Team: The A-1 Heme Team Date: December 1999
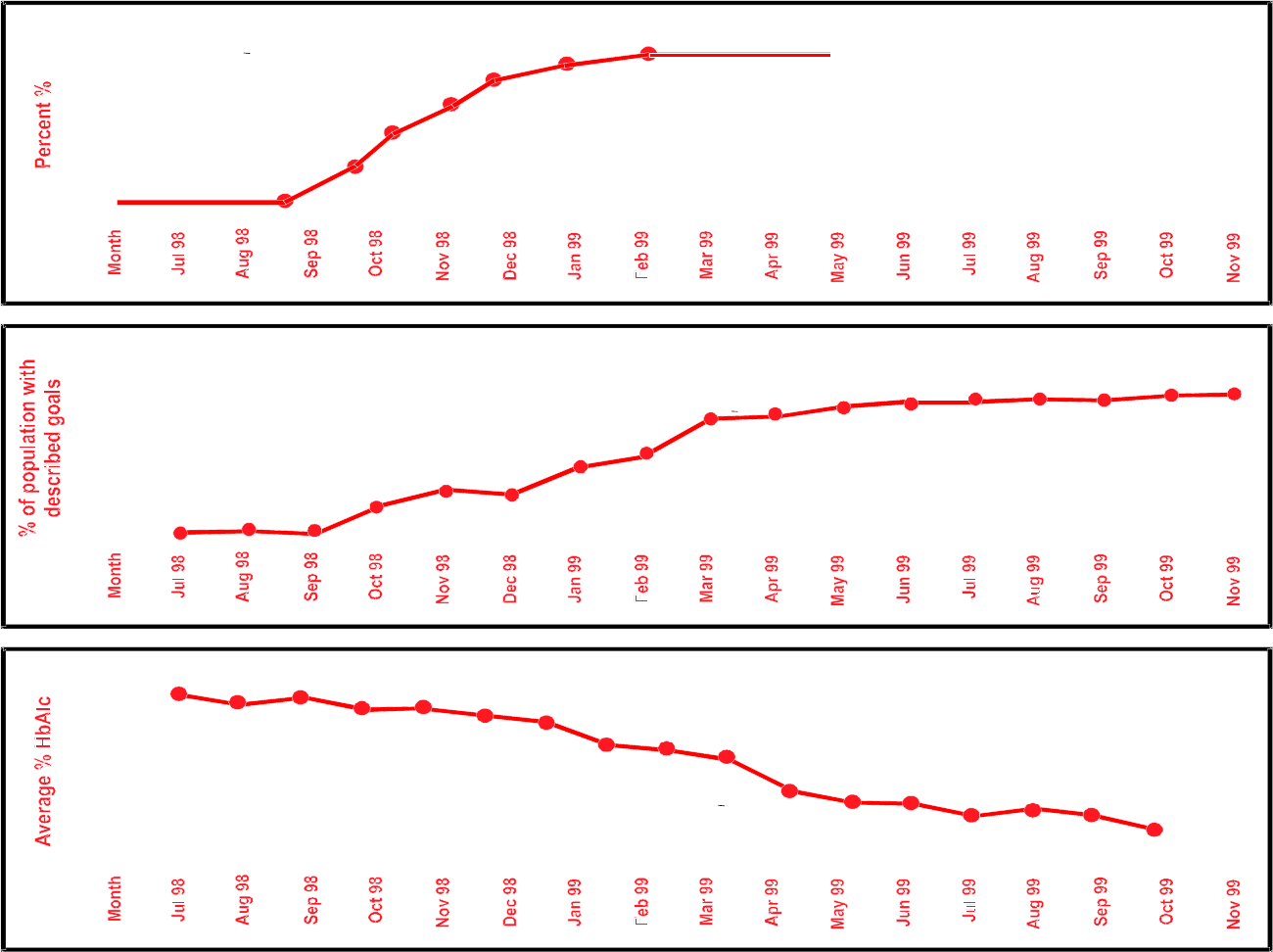
I. Aim: Redesign the practice in all clinics in the health care system so that 70 percent of the diabetes
patients have patient self-management goals and targets, more than 90 percent of patients have an
HbA1c at least bi-annually, 3 months apart, and the average HbA1c levels for the diabetes population
is less than 8.0 percent, and the blood pressure is less than 140/90 for 80% of the diabetes
population.
II. Measures:
1. Percentage of diabetes patients with documented goals and targets.
2. Percent of diabetes patients with 2 HbA1c tests yearly, 3 months apart.
3. Average HbAlc levels of diabetes population based on most recent test.
4. Percent of diabetes patients with documented exercise program.
5. Blood pressure for diabetes population based on the most recent reading.
III. Sampling Plan: Monthly analysis and summary of registry of diabetes patients.
IV. Annotated Graph(s) of Key Measure(s):
V. Brief Description of Changes Tested (annotate on charts):
Key Cycles and Themes from Chronic Care Model
Cycle 1: Establish registry, begin summarizing measures monthly, begin tracking and follow-
up.
Theme: Information System
Cycle 2: Regular meetings of the diabetes care team have begun.
Theme: Practice Re-design
Cycle 3: Offer choices for location and group visits.
Theme: Practice Re-design
Cycle 4: Begin Collaborative goal-setting on visits with diabetes patients.
Theme: Patient Self-management
Cycle 5: Enroll appropriate patients in community weight loss programs.
Theme: Patient Self-management
Cycle 6: Communicate new guidelines for aspirin use.
Theme: Clinical Decision Support
Cycle 7: Implement new procedure for diabetes foot exam.
Theme: Practice Re-design
Cycle 8: Begin intervention program for foot exam for at risk patients.
Theme: Practice Re-design
Cycle 9: Link diabetes patients with community smoking cessation support groups.
Theme: Community Resources/Partnerships
Summary of Results: All aspects of the model for care of patients with diabetes have been
implemented (self-management, decision support, changes in delivery system design, active
8
registry of patients).
Self-Management Support
Target
Cycle 3
Cycle 1
0
20
40
60
80
100
Cycle 2
Cycle 6
Glycemic Control
Target
Cycle 7
Cycle 5
7.0
8
8.5
9
9.5
Cycle 4
Cycle 8
Cycle 9
10
HgA1C Tests
Target
50
60
70
80
90
100
9


