
Fillable Printable Birth Parent Request for Original Birth Certificate from Adoption Sealed File
Fillable Printable Birth Parent Request for Original Birth Certificate from Adoption Sealed File
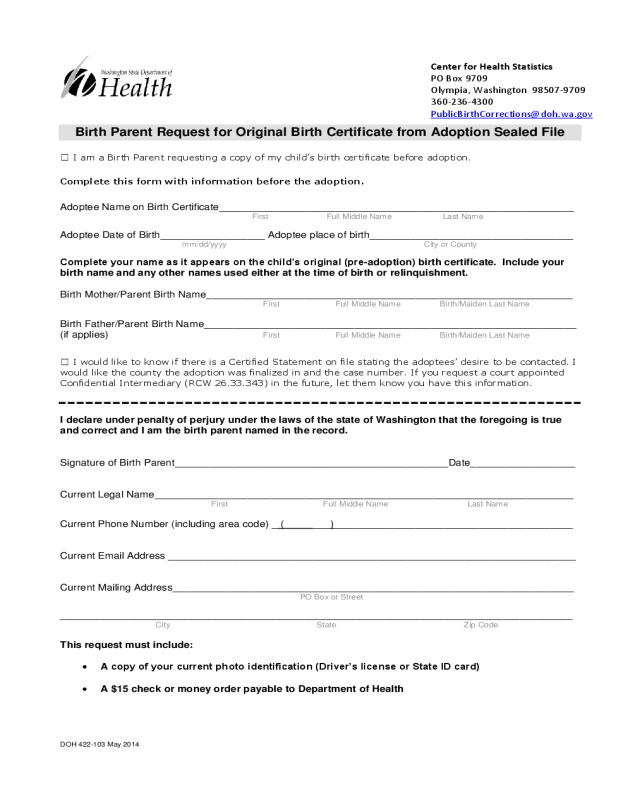
Birth Parent Request for Original Birth Certificate from Adoption Sealed File
DOH 422-103 May 2014
Center for Health Statistics
PO Box 9709
Olympia, Washington 98507-9709
360-236-4300
PublicBirthCorrections@doh.wa.gov
Birth Parent R equest for Original Birth Certificate from Adoption Sealed File
☐ I am a Birth Parent requesting a copy of my child’s birth certificate before adoption.
Complete this form with information before the adoption.
Adoptee Name on Birth Certificate_____________________________________________________________
First Full Middle Name Last Name
Adoptee Date of Birth__________________ Adoptee place of birth___________________________________
mm/dd/yyyy City or County
Complete your name as it appears on the child’s original (pre-adoption) birth certificate. Include your
birth name and any other names used either at the time of birth or relinquishment.
Birth Mother/Parent Birth Name_______________________________________________________________
First Full Middle Name Birth/Maiden Last Name
Birth Father/Parent Birth Name________________________________________________________________
(if applies) First Full Middle Name Birth/Maiden Last Name
☐ I would like to know if there is a Certified Statement on file stating the adoptees’ desire to be contacted. I
would like the county the adoption was finalized in and the case number. If you request a court appointed
Confidential Intermediary (RCW 26.33.343) in the future, let them know you have this information.
I declare under penalty of perjury under the laws of the state of Washington that the foregoing is true
and correct and I am the birth parent named in the record.
Signature of Birth Parent_______________________________________________Date__________________
Current Legal Name________________________________________________________________________
First Full Middle Name Last Name
Current Phone Number (including area code) _ ( ___)_________________________________________
Current Email Address ______________________________________________________________________
Current Mailing Address_____________________________________________________________________
PO Box or Street
________________________________________________________________________________________
City State Zip Code
This request must include:
A copy of your current photo identification (Driver’s license or State ID card)
A $15 check or money order payable to Department of Health


