
Fillable Printable Blank Employee Incident Report Form
Fillable Printable Blank Employee Incident Report Form
Blank Employee Incident Report Form
Fracture
Burns
Bruises
Sprain or Strain
Foreign Body
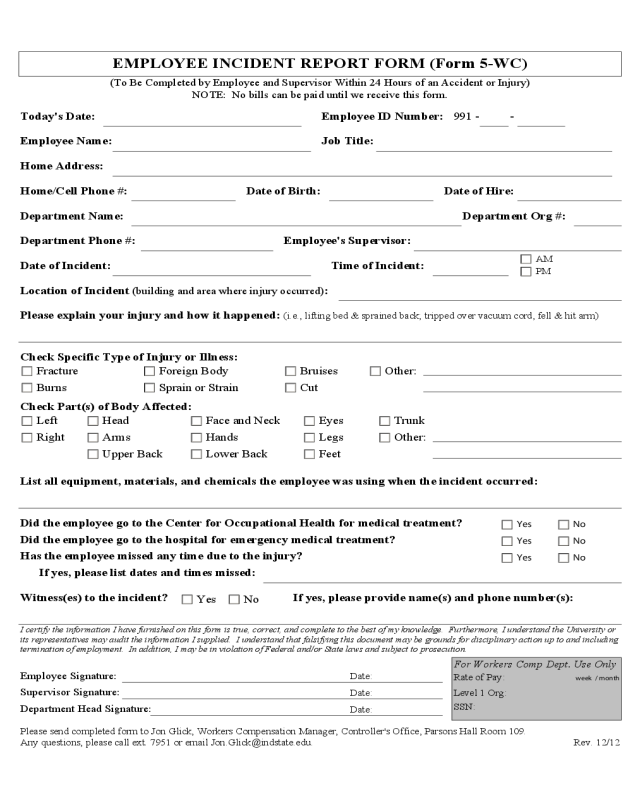
EMPLOYEE INCIDENT REPORT FORM (Form 5-WC)
Other:
Cut
(To Be Completed by Employee and Supervisor Within 24 Hours of an Accident or Injury)
NOTE: No bills can be paid until we receive this form.
Right
Face and NeckLeft
For Workers Comp Dept. Use Only
Rate of Pay:
Today's Date:
Employee Name:
Date of Birth:
Home Address:
Department Phone #:
Department Name:
Date of Incident:
Employee ID Number:
Job Title:
Date of Hire:
Check Specific Type of Injury or Illness:
Check Part(s) of Body Affected:
Department Head Signature:
Employee's Supervisor:
Department Org #:
Time of Incident:
Please send completed form to Jon Glick, Workers Compensation Manager, Controller's Office, Parsons Hall Room 109.
Any questions, please call ext. 7951 or email [email protected].
List all equipment, materials, and chemicals the employee was using when the incident occurred:
Hands Legs
TrunkEyes
Feet
Arms
Head
Other:
Upper Back Lower Back
PM
AM
991 - -
Location of Incident (building and area where injury occurred):
Please explain your injury and how it happened: (i.e., lifting bed & sprained back; tripped over vacuum cord, fell & hit arm)
week / month
SSN:
Level 1 Org:
Date:
Date:
Date:
Home/Cell Phone #:
Supervisor Signature:
Employee Signature:
I certify the information I have furnished on this form is true, correct, and complete to the best of my knowledge. Furthermore, I understand the University or
its representatives may audit the information I supplied. I understand that falsifying this document may be grounds for disciplinary action up to and including
termination of employment. In addition, I may be in violation of Federal and/or State laws and subject to prosecution.
If yes, please provide name(s) and phone number(s):
No Yes
Witness(es) to the incident?
No
No
No
Yes
Yes
Yes
If yes, please list dates and times missed:
Has the employee missed any time due to the injury?
Did the employee go to the hospital for emergency medical treatment?
Did the employee go to the Center for Occupational Health for medical treatment?
Rev. 12/12


