
Fillable Printable Caries Risk Assessment Template
Fillable Printable Caries Risk Assessment Template
Caries Risk Assessment Template
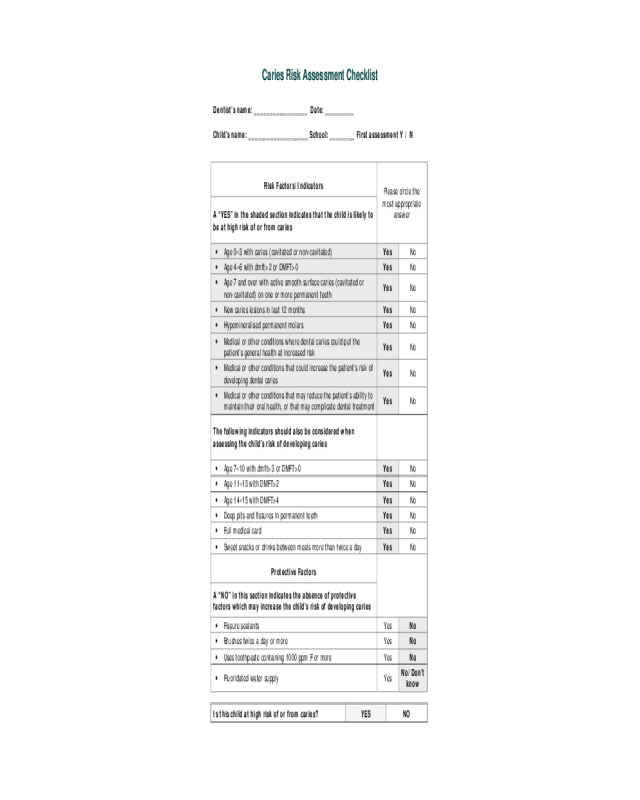
Caries Risk Assessment Checklist
Dentist’s name: _________________ Date: _________
Child’s name: ___________________ School: ________ First assessment Y / N
Risk Factors/Indicators
A “YES” in the shaded section indicates that the child is likely to
be at high risk of or from caries
Please circle the
most appropriate
answer
•Age 0–3 with caries (cavitated or non-cavitated) Yes No
•Age 4–6 with dmft>2 or DMFT>0 Yes No
•Age 7 and over with active smooth surface caries (cavitated or
non-cavitated) on one or more permanent teeth
Yes No
•New caries lesions in last 12 months Yes No
•Hypomineralised permanent molars Yes No
•Medical or other conditions where dental caries could put the
patient’s general health at increased risk
Yes No
•Medical or other conditions that could increase the patient’s risk of
developing dental caries
Yes No
•Medical or other conditions that may reduce the patient’s ability to
maintain their oral health, or that may complicate dental treatment
Yes No
The following indicators should also be considered when
assessing the child’s risk of developing caries
•Age 7–10 with dmft>3 or DMFT>0 Yes No
•Age 11–13 with DMFT>2 Yes No
•Age 14–15 with DMFT>4 Yes No
•Deep pits and fissures in permanent teeth Yes No
•Full medical card Yes No
•Sweet snacks or drinks between meals more than twice a day Yes No
Protective Factors
A “NO” in this section indicates the absence of protective
factors which may increase the child’s risk of developing caries
•Fissure sealants Yes No
•Brushes twice a day or more Yes No
•Uses toothpaste containing 1000 ppm F or more Yes No
•Fluoridated water supply Yes
No/Don’t
know
Is this child at high risk of or from caries? YES NO
Notes on the Caries Risk Assessment Checklist
Introduction
The approach taken dur ing the dev elopment of this checkli st was that all children are at risk of developing caries
but some children are at high risk, and these are the ones we want to identify. The assessment of car ies risk is
something that every dentist does, usually informally or implicitly. The aim of the checklist is to encourage a
formal, systematic approach to identifying individual children who may be at high risk of developing decay.
Caries risk assessment should form the basis of a risk-based approach to patient treatment and recall, with
repeat assessments indicating if the child’s risk status is changing over time.
The checklist is divided into 2 main sections: risk factors/indicators and protective factors. The shaded part
contains the risk factors/indicators that the Guideline Development Group considered most important for
identifying high caries risk c hildren. A score in the shade d part indicates that a child is likely to be at high risk of
or from caries. Other indicators that sh ould be taken into account when assessing the child’s r isk status complete
this section. The second section contains protective factors that should also be considered. The checklist
combines the two most consi stent predictors of future caries: prev ious caries experienc e
23
and the dentist’s own
assessment.
The dentist makes the final decision about ca ries risk status, based on their overall assessment of
the patient. The following notes give some pointers on filling in the checklist.
Risk Factors/Indicators
Age 0–3:Any child un der the age of 4 who sho ws any evidence of car ies – with or without cavitation – should be
considered high risk, as the consequences of any caries for this age group can mean recourse to general
anaesthesia for treatment.
Age 7
and over: Caries is a dynamic process that can progress or arrest. The concept of lesion activity is
becoming increasingly important in assessing a patient’s risk of developing future caries. There is currently no
international consensus on the diagnosis of active lesions, and for the purposes of this checklist, we are
suggesting a modified version of the criteria defined by Nyvad et al. An active lesion is one which is likely to
progress if nothing is done. It is more than just a “white spot” lesion. An active, non cavitated enamel lesion is
characterised by a whitish/yellow opaque surface with loss of lustre and exhibiting a “chalky” appearance.
Inactive lesions tend to be shiny and smooth.
New lesions: New caries in the last 12 mont hs, or progression of non-cavitated les ions (clinical or radiographic)
is a good indicator of high caries activity. It would be a key factor to assess, particularly on repeat caries risk
assessments for children deemed to be high risk.
Smooth surface caries: At least 70% of caries in permanent teeth in Irish children occurs on pit and fissure
surfaces. The occurrence of caries on smo oth surfaces, i.e. proximal, buccal or pal atal (excluding the respective
pits) or lingual surfaces, indicates a different pattern of disease and potentially a greater risk of developing further
decay. The presence of approximal lesio ns on bitewing (if available) should also be considere d when assessing
smooth surface lesions (although it will not b e possibl e to assess the activi t y of the lesion from radio grap hs taken
at a single timepoint).
Hypomineralised molars: Molar hypomineralisation varies in severity, and some hypomineralised molars can
disintegrate rapidly, making early detection and monitoring of these teeth essential. In more severe cases,
hypomineralised molars present a restorative and long-term management challenge. Other developmental
disorders of tooth formation, e.g. amelogenesis imperfecta, which can predispose to caries, should also be
considered in this category.
Deep pits and fissures: The morphology of the occlusal surface has been shown to be a good predictor of
caries risk.
Medical or other conditions: This section considers factors from the medical history that you normal ly take for
your patient, that may put the person at risk of or from caries. Some examples of conditions that could be
included in each of the categories are shown below.
Medical or other conditions Examples
Conditions where dental caries could put th e
patient’s general health at increased risk
Cardiovascular disease
Bleeding disorders
Immunosuppression
Conditions that could increase the patient’s risk of
developing dental caries
Salivary hypofunction
Medications that reduce saliva flo w
Long term use of sugar-containing medic ine
Conditions that may reduce the patient’s abili ty to
maintain their oral health, or that may complicate
dental treatment
Certain physical and intellectual disabilities,
Cleft lip/palate
Anxious*, nervous* or phobic conditions,
Behavioural problems
*Over and above what would be considered “normal” anxiety or nervousness for children
DMFT (Decayed/Missing/Filled Teeth): In calculating dmft/DMFT, only teeth that have been extracted due to
caries should be counted as missing. Similarly, only fillings that have been placed due to caries should be
counted. The DMFT cut-offs in the checklist are based onthe mean DMFT of the top one third of children with
the highest caries levels from the North South surve y. In the North South survey, caries was recorded without the
use of (bitewing) radiographs; therefore caries detected on (bitewing) radiographs sh ould not be included in the
dmft/DMFT calculation.
Dietary habits: Diet is one of the main risk factors for dental cari es, and it can be the most difficult and sensitive
area on which to get acc urate information. We are sug gesting that the q uestion could be phrased along the line s
of the question on diet that was included in the North South surve y.
Dietary habits Suggested question
Sweet snacks or drinks between
meals more than twice a day
How often does your child eat sweet food or drinks e.g.
biscuits, cakes, sweets, fizzy drinks/squash, fruit drinks etc
between normal meals?
Medical Card: There is fairly strong evi dence of an inverse relationship bet ween socio-ec onomic status and or al
health in children under 12 years of age. Medical card status has been used in Irish studies as an indicator of
disadvantage. Medical card status may be a particularly useful indicator of caries risk where children are too
young for their risk to be based on caries history. Since the introduction of the GP Visit card, which has higher
income thresholds for eligibilit y, it is necessary to establish if the patient has a Full medical card. V ery often this
data is collected as part of the medical history or patient details, and data from these sources can be used to
complete the checklist.
Protective Factors
The effectiveness of the protective factors listed in the checklist at reducing caries has been established in
various systematic reviews. The absence of protective factors could increa se a child’s risk of developing caries.


