
Fillable Printable Child Care Staff Health Assessment - Pennsylvania
Fillable Printable Child Care Staff Health Assessment - Pennsylvania
Child Care Staff Health Assessment - Pennsylvania
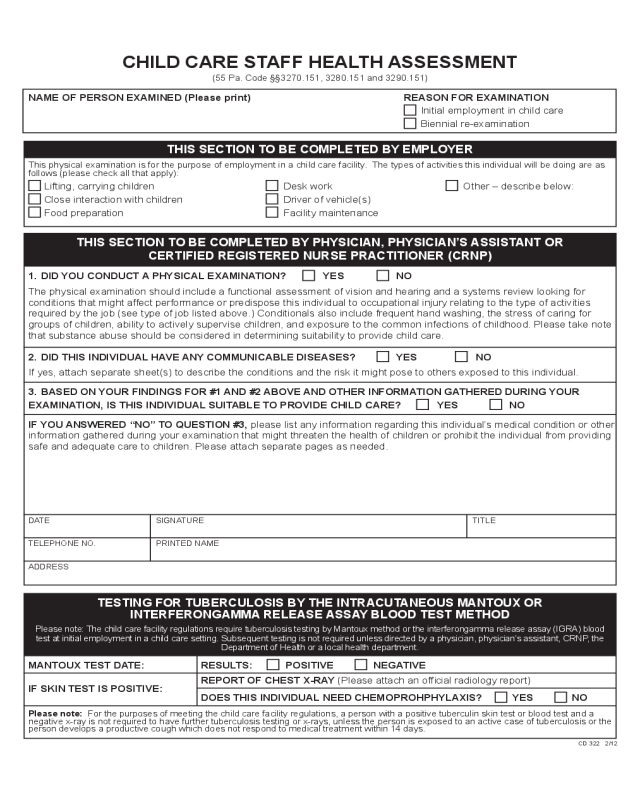
CHILD CARE STAFF HEALTH ASSESSMENT
(55 Pa. Code §§3270.151, 3280.151 and 3290.151)
NAME OF PERSON EXAMINED (Please print) REASON FOR EXAMINATION
Initial employment in child care
Biennial re-examination
THIS SECTION TO BE COMPLETED BY EMPLOYER
This physical examination is for the purpose of employment in a child care facility. The types of activities this individual will be doing are as
follows (please check all that apply):
Lifting, carrying children Desk work Other – describe below:
Close interaction with children Driver of vehicle(s)
Food preparation Facility maintenance
THIS SECTION TO BE COMPLETED BY PHYSICIAN, PHYSICIAN’S ASSISTANT OR
CERTIFIED REGISTERED NURSE PRACTITIONER (CRNP)
1. DID YOU CONDUCT A PHYSICAL EXAMINATION? YES NO
The physical examination should include a functional assessment of vision and hearing and a systems review looking for
conditions that might affect performance or predispose this individual to occupational injury relating to the type of activities
required by the job (see type of job listed above.) Conditionals also include frequent hand washing, the stress of caring for
groups of children, ability to actively supervise children, and exposure to the common infections of childhood. Please take note
that substance abuse should be considered in determining suitability to provide child care.
2. DID THIS INDIVIDUAL HAVE ANY COMMUNICABLE DISEASES? YES NO
If yes, attach separate sheet(s) to describe the conditions and the risk it might pose to others exposed to this individual.
3. BASED ON YOUR FINDINGS FOR #1 AND #2 ABOVE AND OTHER INFORMATION GATHERED DURING YOUR
EXAMINATION, IS THIS INDIVIDUAL SUITABLE TO PROVIDE CHILD CARE? YES NO
IF YOU ANSWERED “NO” TO QUESTION #3, please list any information regarding this individual’s medical condition or other
information gathered during your examination that might threaten the health of children or prohibit the individual from providing
safe and adequate care to children. Please attach separate pages as needed.
DATE SIGNATURE TITLE
TELEPHONE NO. PRINTED NAME
ADDRESS
TESTING FOR TUBERCULOSIS BY THE INTRACUTANEOUS MANTOUX OR
INTERFERONGAMMA RELEASE ASSAY BLOOD TEST METHOD
Please note: The child care facility regulations require tuberculosis testing by Mantoux method or the interferongamma release assay (IGRA) blood
test at initial employment in a child care setting. Subsequent testing is not required unless directed by a physician, physician’s assistant, CRNP, the
Department of Health or a local health department.
MANTOUX TEST DATE: RESULTS: POSITIVE NEGATIVE
IF SKIN TEST IS POSITIVE:
REPORT OF CHEST X-RAY (Please attach an ofcial radiology report)
DOES THIS INDIVIDUAL NEED CHEMOPROHPHYLAXIS? YES NO
Please note: For the purposes of meeting the child care facility regulations, a person with a positive tuberculin skin test or blood test and a
negative x-ray is not required to have further tuberculosis testing or x-rays, unless the person is exposed to an active case of tuberculosis or the
person develops a productive cough which does not respond to medical treatment within 14 days.
CD 322 2/12


