
Fillable Printable Dental Insurance Verification Form - Alaska
Fillable Printable Dental Insurance Verification Form - Alaska
Dental Insurance Verification Form - Alaska
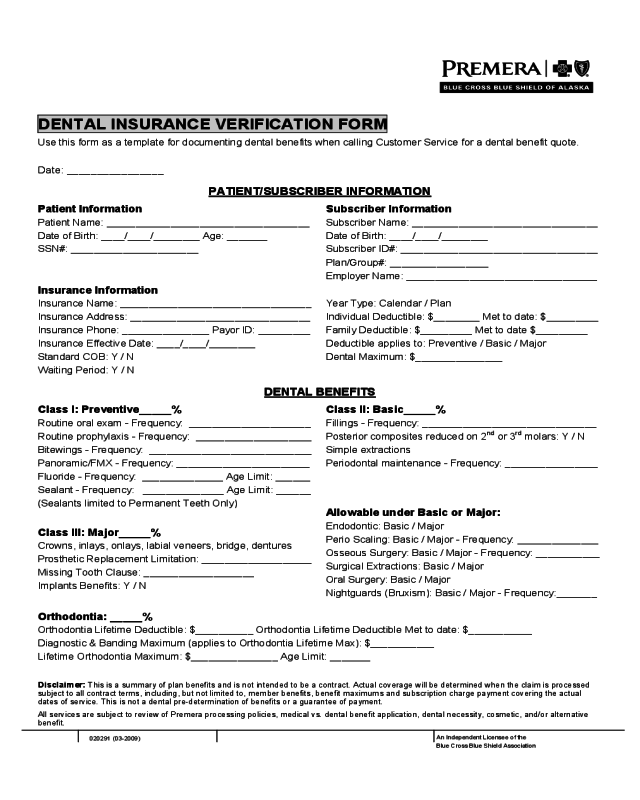
DENTAL INSURANCE VERIFICATION FORM
Use this form as a template for documenting dental benefits when calling Customer Service for a dental benefit quote.
Date: ________________
PATIENT/SUBSCRIBER INFORMATION
Patient Information Subscriber Information
Patient Name: ___________________________________ Subscriber Name: ________________________________
Date of Birth: ____/____/________ Age: _______ Date of Birth: ____/____/________
SSN#: ______________________ Subscriber ID#: __________________________________
Plan/Group#: _________________
Employer Name: _________________________________
Insurance Information
Insurance Name: _________________________________ Year Type: Calendar / Plan
Insurance Address: _______________________________ Individual Deductible: $________ Met to date: $_________
Insurance Phone: _______________ Payor ID: _________ Family Deductible: $_________ Met to date $_________
Insurance Effective Date: ____/____/________ Deductible applies to: Preventive / Basic / Major
Standard COB: Y / N Dental Maximum: $_______________
Waiting Period: Y / N
DENTAL BENEFITS
Class I: Preventive_____% Class II: Basic_____%
Routine oral exam - Frequency: _____________________ Fillings - Frequency: ______________________________
Routine prophylaxis - Frequency: ____________________
Bitewings - Frequency: ____________________________
Panoramic/FMX - Frequency: _______________________
Fluoride - Frequency: ______________ Age Limit: ______
Sealant - Frequency: ______________ Age Limit: ______
(Sealants limited to Permanent Teeth Only)
Class III: Major_____%
Crowns, inlays, onlays, labial veneers, bridge, dentures
Prosthetic Replacement Limitation: ___________________
Missing Tooth Clause: ___________________
Implants Benefits: Y / N
Posterior composites reduced on 2
nd
or 3
rd
molars: Y / N
Simple extractions
Periodontal maintenance - Frequency: ________________
Allowable under Basic or Major:
Endodontic: Basic / Major
Perio Scaling: Basic / Major - Frequency: ______________
Osseous Surgery: Basic / Major - Frequency: ___________
Surgical Extractions: Basic / Major
Oral Surgery: Basic / Major
Nightguards (Bruxism): Basic / Major - Frequency:_______
Orthodontia: _____%
Orthodontia Lifetime Deductible: $__________ Orthodontia Lifetime Deductible Met to date: $___________
Diagnostic & Banding Maximum (applies to Orthodontia Lifetime Max): $___________
Lifetime Orthodontia Maximum: $_______________ Age Limit: _______
Disclaimer:
This is a summary of plan benefits and is not intended to be a contract. Actual coverage will be determined when the claim is processed
subject to all contract terms, including, but not limited to, member benefits, benefit maximums and subscription charge payment covering the actual
dates of service. This is not a dental pre-determination of benefits or a guarantee of payment.
All services are subject to review of Premera processing policies, medical vs. dental benefit application, dental necessity, cosmetic, and/or alternative
benefit.
An Independent Licensee of the
Blue Cross Blue Shield Association
020291 (03-2009)


