
Fillable Printable Dependent Care/ Health Care Reimbursement Account Plans Claim Form
Fillable Printable Dependent Care/ Health Care Reimbursement Account Plans Claim Form
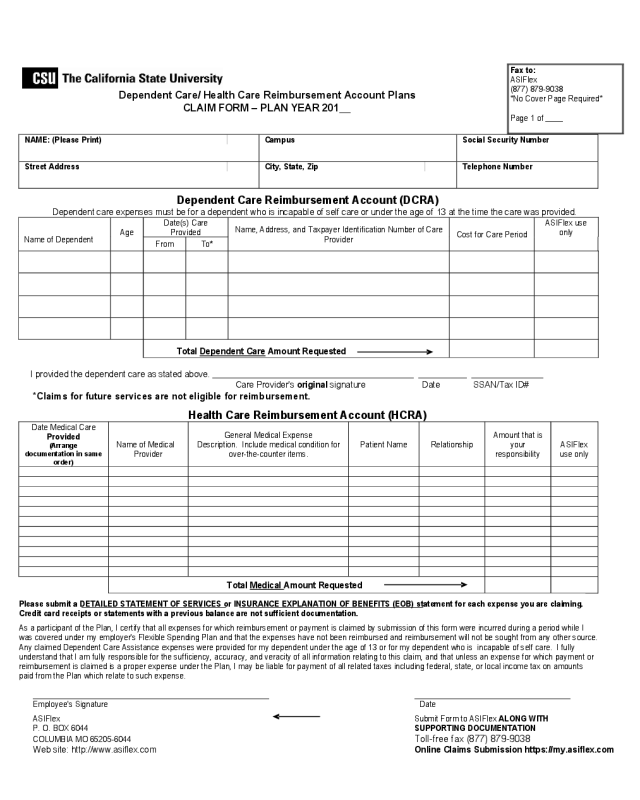
Dependent Care/ Health Care Reimbursement Account Plans Claim Form
NAME: (Please Print)
Campus
Social Security Number
Street Address
City, State, Zip
Telephone Number
Dependent Care Reimbursement Account (DCRA)
Dependent care expenses must be for a dependent who is incapable of self care or under the age of 13 at the time the care was provided.
Name of Dependent
Age
Date(s) Care
Provided
Name, Address, and Taxpayer Identification Number of Care
Provider
Cost for Care Period
ASIFlex use
only
From To*
Total Dependent Care Amount Requested
I provided the dependent care as stated above. __________________________________________ __________ _______________
Care Provider's original signature Date SSAN/Tax ID#
*Claims for future services are not eligible for reimbursement.
Health Care Reimbursement Account (HCRA)
Date Medical Care
Provided
(Arrange
documentation in same
order)
Name of Medical
Provider
General Medical Expense
Description. Include medical condition for
over-the-counter items.
Patient Name Relationship
Amount that is
your
responsibility
ASIFlex
use only
Total Medical Amount Requested
Please submit a DETAILED STATEMENT OF SERVICES or INSURANCE EXPLANATION OF BENEFITS (EOB) statement for each expense you are claiming.
Credit card receipts or statements with a previous balance are not sufficient documentation.
As a participant of the Plan, I certify that all expenses for which reimbursement or payment is claimed by submission of this form were incurred during a period while I
was covered under my employer's Flexible Spending Plan and that the expenses have not been reimbursed and reimbursement will not be sought from any other source.
Any claimed Dependent Care Assistance expenses were provided for my dependent under the age of 13 or for my dependent who is incapable of self care. I fully
understand that I am fully responsible for the sufficiency, accuracy, and veracity of all information relating to this claim, and that unless an expense for which payment or
reimbursement is claimed is a proper expense under the Plan, I may be liable for payment of all related taxes including federal, state, or local income tax on amounts
paid from the Plan which relate to such expense.
__________________________________________________ _________________________________
Employee's Signature Date
ASIFlex Submit Form to ASIFlex ALONG WITH
P. O. BOX 6044 SUPPORTING DOCUMENTATION
COLUMBIA MO 65205-6044
Toll-free fax (877) 879-9038
Web site: http://www.asiflex.com Online Claims Submission https://my.asiflex.com
Fax to:
ASIFlex
(877) 879-9038
*No Cover Page Required*
Page 1 of ____
Dependent Care/ Health Care Reimbursement Account Plans
CLAIM FORM – PLAN YEAR 201__
Claim Filing Requirements
1.
Print your name, address, and social security number.
2.
List expenses by date & arrange the supporting statements in the same order. Please circle the service dates on your
documentation. If you have several statements from the same provider, you may subtotal them and list them on one line with a range of
dates.
Day care claims - complete the DCRA section
Health care claims - complete the HCRA section (The amount column should be the amount you are requesting after any
insurance payment or provider discount for each expense).
3.
Enclose required documentation
*
. A written statement from the dependent care or medical (Dr., hospital, pharmacy, etc.) provider of
the service or an insurance company benefits statement showing all of the following:
The name of the dependent care or medical service provider,
The date or range of dates of medical service or day care. Although this date may be the same as the date paid it must be
clear on what date the service was provided. The services must have already been provided.
A description of the service provided (for example, for health care, "dental cleaning", or for day care "day care"),
The name of the person or persons receiving the medical or dependent care, and
The cost of the service, not just the amount paid.
*
Dependent Care claims only” - You may either provide documentation from the day care provider or have the provider complete
the DCRA, then sign on the "Provider's Signature" line and date the signature. You do not need to do both.
Requests filed without the above documentation cannot be processed and will be returned.
4.
Sign the claim form.
5.
Keep copies for your tax records.
6.
Mail to the address on the front of this form, submit the claim online, or Fax to (877) 879-9038. This is a toll-free number but employee
use of an office fax machine may not be appropriate. Please check with your employer before using an office fax machine.
Claim forms: You may copy this form or obtain forms online at http://www.asiflex.com
Medical equipment: Requires a letter from a physician every 12 months stating the nature of your medical condition, the specific equipment
needed and that the equipment is essential to the treatment.
Over-the-counter medicines & drugs: Effective January 1, 2011, over-the-counter (OTC) medicines will not be reimbursable unless you
have a valid prescription. Insulin still qualifies for reimbursement without a prescription. Equipment, supplies, and diagnostic devices such as
bandages, hearing aid batteries, blood sugar test kits, etc. will remain eligible for reimbursement without a prescription. Please refer to ASIFlex’s
Website, http://www.asiflex.com, for a list of OTC medicine categories that no longer qualify for reimbursement without a prescription after January
1, 2011. To claim vitamins, herbs or nutritional supplements, you must have a written diagnosis of the medical condition and “prescription” of all
specific items for that condition on file with the claims office. You must renew this physician notice every 12 months and file it with the claims office
with the first claim submitted for those items each plan year.
Online Claims Submission: In order to submit claims online, you must 1) have high-speed internet access, 2) be able to scan your supporting
documentation into one or more PDF files that are less than 812K (8MB) in size each, and 3) know your P.I.N., which you can find on your
enrollment confirmation, or you may obtain by calling ASIFlex’s customer service center (800) 659-3035. The website for online claims submission
is https://my.asiflex.com. Emailed claims will not be accepted.
Resources
Customer Service: (800) 659-3035 Toll-Free Claims Fax: (877) 879-9038
Customer Service Email:
asi@asiflex.com
Customer Service Website:
www.asiflex.com
Online claims submission:
https://my.asiflex.com
Claims mailing address: P.O. Box 6044
Columbia, MO 65205
Orthodontics: Requests may be reimbursed for a reasonable monthly payment on or after the payment is due and paid. The payment must be a
reasonable approximation of the value of each month's service. You may only file claims for orthodontic payments while treatment is in process.
You must submit a paid receipt from your orthodontist or a photocopy of the monthly coupon and your check. Pre-payments are not allowed. You
must submit a written statement from the orthodontist showing the charge for the initial installation work, when it was completed and a paid receipt
to claim an initial down payment or appliance fee.
Claims payment and account information is available 24 hours a day 7 days a week: View complete history including available funds online at
ASIFlex’s customer service center (800) 659-3035.
www.asiflex.com (Account Detail). You will need your P.I.N., which you can find on your enrollment confirmation, or you may obtain by calling


