
- Georgia's Own Direct Deposit Form - Georgia
- Direct Deposit Request - Alabama
- Direct Deposit Authorization Agreement Form - Illinois
- Ach Form for Direct Deposit Payments to Providers - Colorado
- Direct Deposit Application Form - Tennessee
- Direct Deposit Authorization Form for Payroll and Expense Reimbursement - Indiana
Fillable Printable Direct Deposit Enrollment or Change Form
Fillable Printable Direct Deposit Enrollment or Change Form
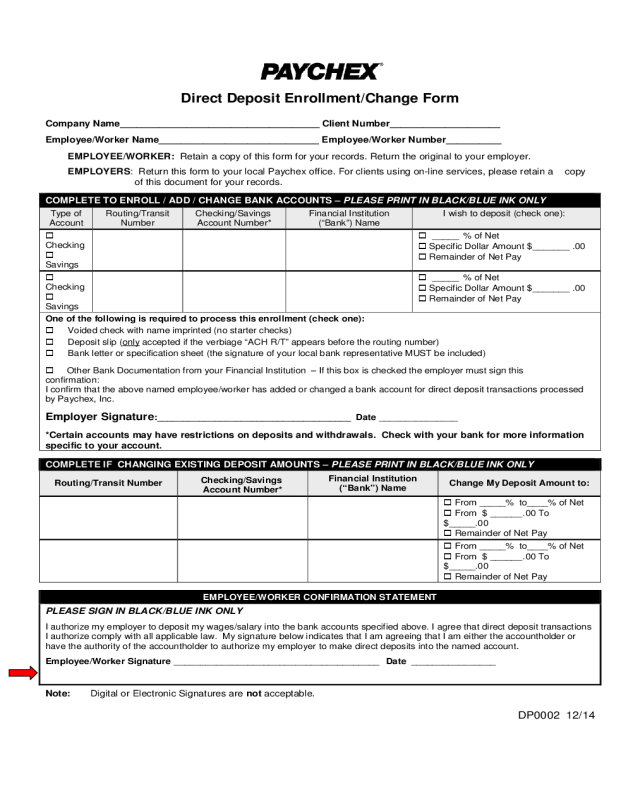
Direct Deposit Enrollment or Change Form
Direct Depos it Enrollment/Cha nge Form
Company Name____________________________________ Client Number____________________
Employee/Worker Name_____________________________ Employee/Worker Number__________
EMPLOYEE/WORKER: Retain a copy of this form for your records. Return the original to your employer.
EMPLOYERS: Return this form to your local Paychex office. For clients using on-line services, please retain a copy
of this document for your records.
COMPLETE TO ENROLL / ADD / CHANGE BANK ACCOUNTS – PLEASE PRINT IN BLACK/BLUE INK ONLY
Type of
Account
Routing/Transit
Number
Checking/Savings
Account Number*
Financial Institut ion
(“Bank ”) Name
I wish to deposit (check one):
Checking
Savings
_____ % of Net
Specific Dollar Amount $ _______ .00
Remainder of Net Pay
Checking
Savings
_____ % of Net
Specific Dollar Amount $ _______ .00
Remainder of Net Pay
One of the following is required to process this enrollment (check one):
Voided check with name imprinted (no starter checks)
Deposit slip (only accepted if the verbiage “ACH R/T” appears before the routing number)
Bank letter or specification sheet (the signature of your local bank representative MUST be inc luded)
Other Bank Documentation from your Financial Institution – If this box is checked the em ployer must sign this
confirmation:
I confirm that the above named employee/worker has added or changed a bank account for direct deposit transactions processed
by Paychex, Inc.
Employer Signat ur e:_____________________________________ Date _______________
*Certain accounts may have restrictions on de posits and withdrawals. Check with your bank for more i nfor mation
specific to your account.
COMPLETE IF CHANGING EXISTING DEPOSIT AMOUNTS – PLE ASE PRINT IN BLACK/BLUE INK ONLY
Routing/Tra nsit Number
Checking/Savings
Ac count Number*
Financial Institution
(“Bank”) Name
Change My Deposit Amount to:
From _____% to____% of N et
From $ ______ .00 To
$_____.00
Remainder of Net Pay
From _____% to____% of N et
From $ ______ .00 To
$_____.00
Remainder of Net Pay
EMPLOYEE/WORKER CONFIRMATION STATEM E NT
PLEASE SIGN IN BLACK/BLUE INK ON LY
I authorize my employer to deposit my wages/salary into the bank accounts specified above. I agree that direct depos i t transactions
I authorize com ply w ith all appl icab le law . My signature below indicates that I am agreeing that I am either the accountholder or
have the authority of the accountholder to authorize my em ployer to make direct deposits into the named account.
Employee/Worker Signature _______________________________________ Date ________________
Note: Digital or Electronic Signatures are not acceptable.
DP0002 12/14


