
Fillable Printable Employee Declaration Form - New Mexico
Fillable Printable Employee Declaration Form - New Mexico
Employee Declaration Form - New Mexico
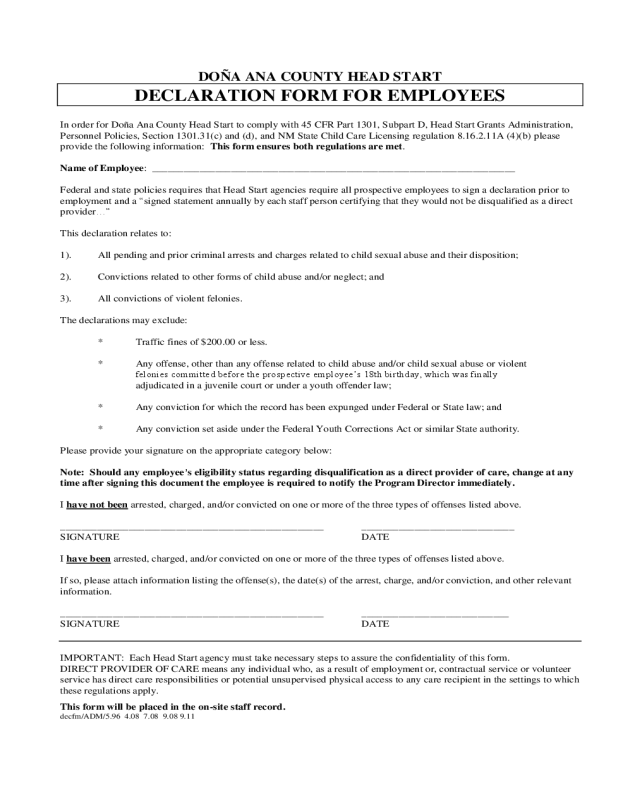
DOÑA ANA COUNTY HEAD START
DECLARATION FORM FOR EMPLOYEES
In order for Doña Ana County Head Start to comply with 45 CFR Part 1301, Subpart D, Head Start Grants Administration,
Personnel Policies, Section 1301.31(c) and (d), and NM State Child Care Licensing regulation 8.16.2.11A (4)(b) please
provide the following information: This form ensures both regulations are met.
Name of Employee: _____________________________________________________________________
Federal and state policies requires that Head Start agencies require all prospective employees to sign a declaration prior to
employment and a “signed statement annually by each staff person certifying that they would not be disqualified as a direct
provider…”
This declaration relates to:
1). All pending and prior criminal arrests and charges related to child sexual abuse and their disposition;
2). Convictions related to other forms of child abuse and/or neglect; and
3). All convictions of violent felonies.
The declarations may exclude:
* Traffic fines of $200.00 or less.
* Any offense, other than any offense related to child abuse and/or child sexual abuse or violent
felonies committed before the prospective employee’s 18th birthday, which was finally
adjudicated in a juvenile court or under a youth offender law;
* Any conviction for which the record has been expunged under Federal or State law; and
* Any conviction set aside under the Federal Youth Corrections Act or similar State authority.
Please provide your signature on the appropriate category below:
Note: Should any employee’s eligibility status regarding disqualification as a direct provider of care, change at any
time after signing this document the employee is required to notify the Program Director immediately.
I have not been arrested, charged, and/or convicted on one or more of the three types of offenses listed above.
__________________________________________________ _____________________________
SIGNATURE DATE
I have been arrested, charged, and/or convicted on one or more of the three types of offenses listed above.
If so, please attach information listing the offense(s), the date(s) of the arrest, charge, and/or conviction, and other relevant
information.
__________________________________________________ ____________________________
SIGNATURE DATE
IMPORTANT: Each Head Start agency must take necessary steps to assure the confidentiality of this form.
DIRECT PROVIDER OF CARE means any individual who, as a result of employment or, contractual service or volunteer
service has direct care responsibilities or potential unsupervised physical access to any care recipient in the settings to which
these regulations apply.
This form will be placed in the on-site staff record.
decfm/ADM/5.96 4.08 7.08 9.08 9.11


