
Fillable Printable Enrollment Form - Washington
Fillable Printable Enrollment Form - Washington
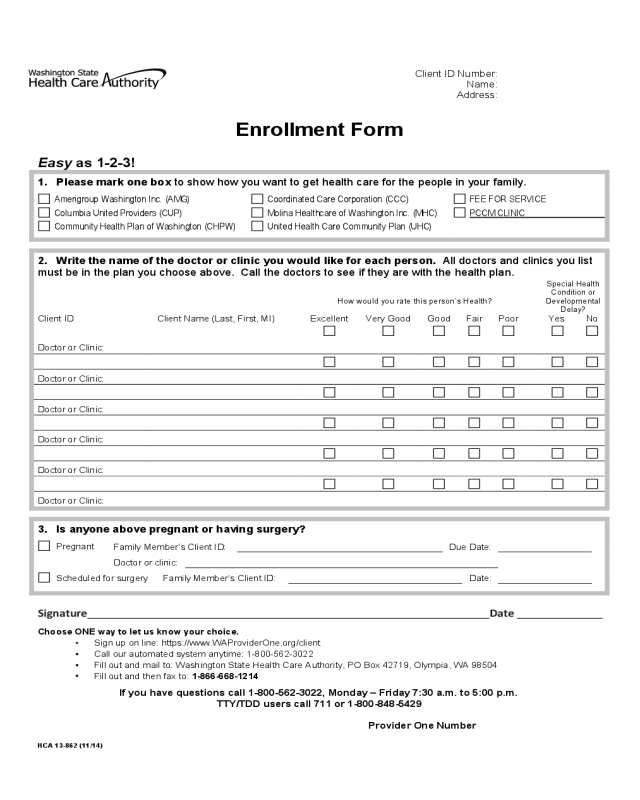
Enrollment Form - Washington

Client ID Number:
Name:
Address:
Enrollment Form
<<secondary form title, as required>>
Easy as 1-2-3!
1. Please mark one box to show how you want to get health care for the people in your family.
Amerigroup Washington Inc. (AMG)
Columbia United Providers (CUP)
Community Health Plan of Washington (CHPW)
Coordinated Care Corporation (CCC)
Molina Healthcare of Washington Inc. (MHC)
United Health Care Community Plan (UHC)
FEE FOR SERVICE
PCCM CLINIC
2. Write the name of the doctor or clinic you would like for each person. All doctors and clinics you list
must be in the plan you choose above. Call the doctors to see if they are with the health plan.
How would you rate this person’s Health?
Special Health
Condition or
Developmental
Delay?
Client ID Client Name (Last, First, MI) Excellent Very Good Good Fair Poor
Yes No
Doctor or Clinic:
Doctor or Clinic:
Doctor or Clinic:
Doctor or Clinic:
Doctor or Clinic:
Doctor or Clinic:
3. Is anyone above pregnant or having surgery?
Pregnant
Family Member’s Client ID:
Due Date:
Doctor or clinic:
Scheduled for surgery
Family Member’s Client ID:
Date:
Signature Date
Choose ONE way to let us know your choice.
•
Sign up on line: https://www.WAProviderOne.org/client
•
Call our automated system anytime: 1-800-562-3022
•
Fill out and mail to: Washington State Health Care Authority, PO Box 42719, Olympia, WA 98504
•
Fill out and then fax to: 1-866-668-1214
If you have questions call 1-800-562-3022, Monday – Friday 7:30 a.m. to 5:00 p.m.
TTY/TDD users call 711 or 1-800-848-5429
Provider One Number<insert HOHP1>
HCA 13-862 (11/14)


