
Fillable Printable Federal Perkins (NDSL) Student Loan Request for Deferment
Fillable Printable Federal Perkins (NDSL) Student Loan Request for Deferment
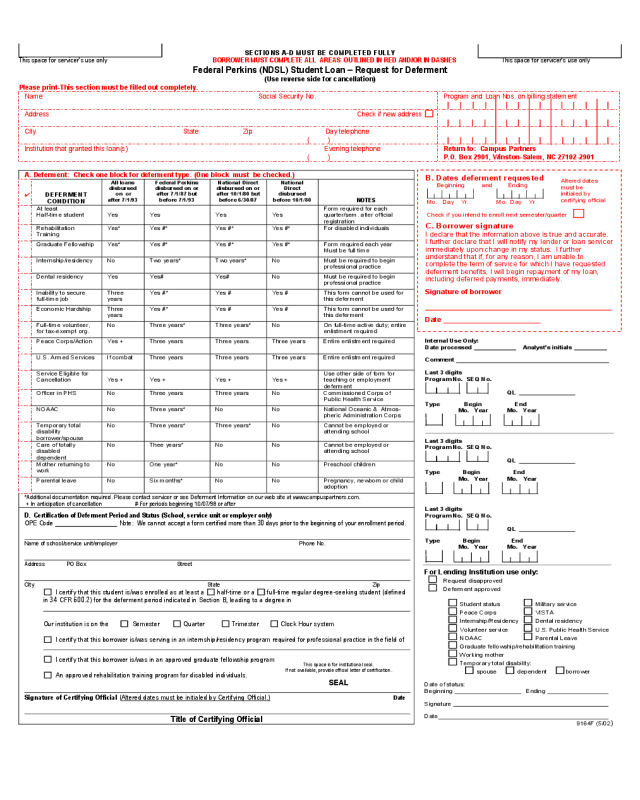
Federal Perkins (NDSL) Student Loan Request for Deferment
SECTIONS A-D MUST BE COMPLETED FULLY
This space for servicer’s use only BORROWER MUST COMPLETE ALL AREAS OUTLINED IN RED AND/OR IN DASHES This space for servicer’s use only
Federal Perkins (NDSL) Student Loan – Request for Deferment
(Use reverse side for cancellation)
Please print-This section must be filled out completely.
Name Social Security No. Program and Loan Nos. on billing statement
Address Check if new address
City State Zip Day telephone
( )
Institution that granted this loan(s) Evening telephone
( )
Return to: Campus Partners
P.O. Box 2901, Winston-Salem, NC 27102-2901
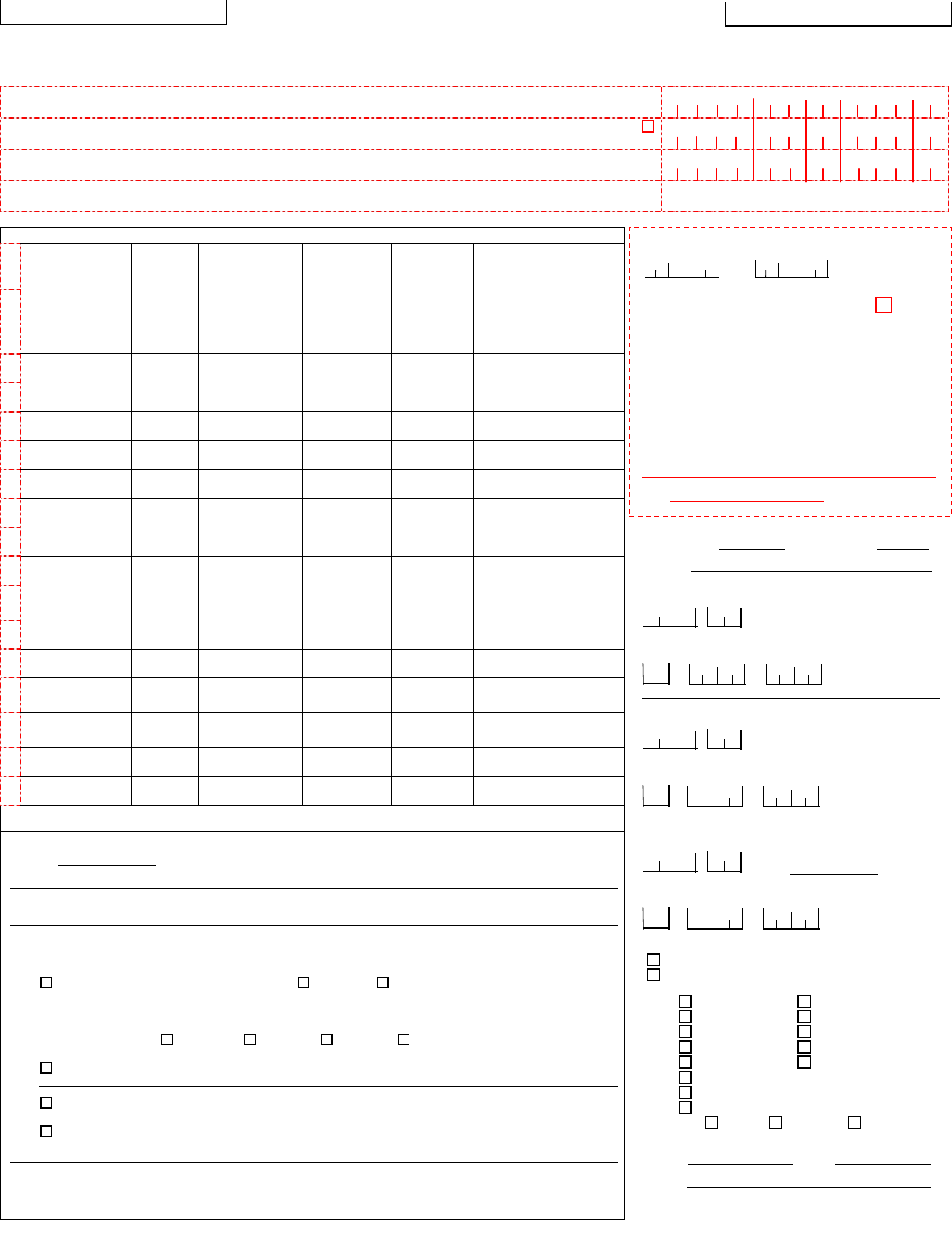
A. Deferment: Check one block for deferment type. (One block must be checked.)
✔
DEFERMENT
CONDITION
All loans
disbursed
on or
after 7/1/93
Federal Perkins
disbursed on or
after 7/1/87 but
before 7/1/93
National Direct
disbursed on or
after 10/1/80 but
before 6/30/87
National
Direct
disbursed
before 10/1/80
NOTES
At least
Half-time student Yes Yes Yes Yes
Form required for each
quarter/sem. after official
registration
Rehabilitation
Training
Yes* Yes #* Yes #* Yes #* For disabled individuals
Graduate Fellowship Yes* Yes #* Yes #* Yes #* Form required each year
Must be full time
Internship/residency No Two years* Two years* No Must be required to begin
professional practice
Dental residency Yes Yes# Yes# No Must be required to begin
professional practice
Inability to secure
full-time job
Three
years
Yes #* Yes # Yes # This form cannot be used for
this deferment
Economic Hardship Three
years
Yes #* Yes # Yes # This form cannot be used for
this deferment
Full-time volunteer,
for tax-exempt org.
No Three years* Three years* No On full-time active duty; entire
enlistment required
Peace Corps/Action Yes + Three years Three years Three years Entire enlistment required
U.S. Armed Services If combat Three years Three years Three years Entire enlistment required
Service Eligible for
Cancellation Yes + Yes + Yes + Yes +
Use other side of form for
teaching or employment
deferment
Officer in PHS No Three years Three years No Commissioned Corps of
Public Health Service
NOAAC No Three years* No No National Oceanic & Atmos-
pheric Administration Corps
Temporary total
disability
borrower/spouse
No Three years* Three years* No Cannot be employed or
attending school
Care of totally
disabled
dependent
No Thee years* No No Cannot be employed or
attending school
Mother returning to
work
No One year* No No Preschool children
Parental leave No Six months* No No Pregnancy, newborn or child
adoption
*Additional documentation required. Please contact servicer or see Deferment Information on our web site at www.campuspartners.com.
+ In anticipation of cancellation # For periods beginning 10/07/98 or after
D. Certification of Deferment Period and Status (School, service unit or employer only)
OPE Code
Note: We cannot accept a form certified more than 30 days prior to the beginning of your enrollment period.
Name of school/service unit/employer Phone No.
Address PO Box Street
City State Zip
I certify that this student is/was enrolled as at least a half-time or a full-time regular degree-seeking student (defined
in 34 CFR 600.2) for the deferment period indicated in Section B, leading to a degree in
Our institution is on the Semester Quarter Trimester Clock Hour system
I certify that this borrower is/was serving in an internship/residency program required for professional practice in the field of
I certify that this borrower is/was in an approved graduate fellowship program.
An approved rehabilitation training program for disabled individuals.
Signature of Certifying Official (Altered dates must be initialed by Certifying Official.) Date
Title of Certifying Official
B. Dates deferment requested
Beginning and Ending
Mo. Day Yr. Mo. Day Yr.
Check if you intend to enroll next semester/quarter
C. Borrower signature
I declare that the information above is true and accurate.
I further declare that I will notify my lender or loan servicer
immediately upon change in my status. I further
understand that if, for any reason, I am unable to
complete the term of service for which I have requested
deferment benefits, I will begin repayment of my loan,
including deferred payments, immediately.
Signature of borrower
Date
A
ltered dates
must be
initialed by
certifying official
Internal Use Only:
Date processed Analyst’s initials
Comment
Last 3 digits
Program No. SEQ No.
QL
Type Begin End
Mo. Year Mo. Year
Last 3 digits
Program No. SEQ No.
QL
Type Begin End
Mo. Year Mo. Year
Last 3 digits
Program No. SEQ No.
QL
Type Begin End
Mo. Year Mo. Year
For Lending Institution use only:
Request disapproved
Deferment approved
Student status Military service
Peace Corps VISTA
Internship/Residency Dental residency
Volunteer service U.S. Public Health Service
NOAAC Parental Leave
Graduate fellowship/rehabilitation training
Working mother
Temporary total disability:
spouse dependent borrower
Date of status:
Beginning Ending
Signature
Date
9164F (5/02)
This space is for institutional seal.
If not available, provide official letter of certification.
SEAL


