
Fillable Printable Form 4162
Fillable Printable Form 4162
Form 4162
Page 1 of 1
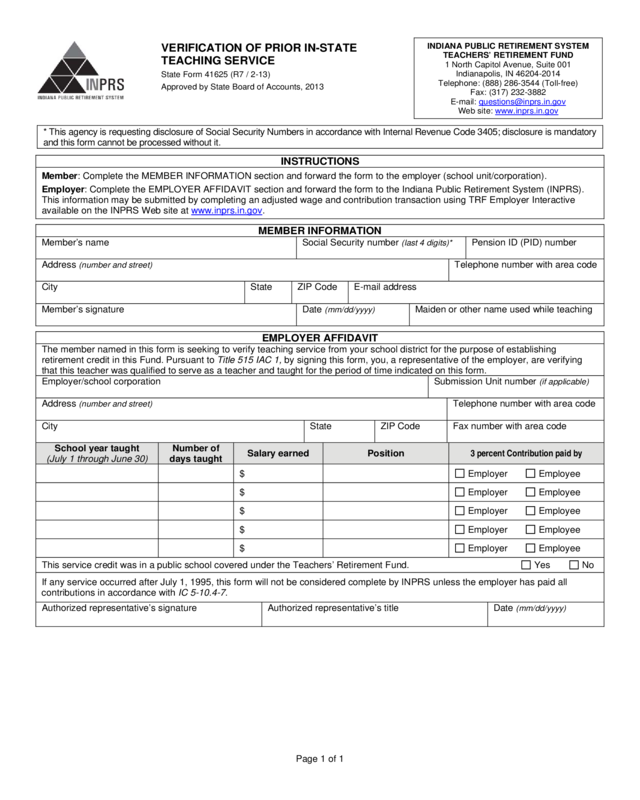
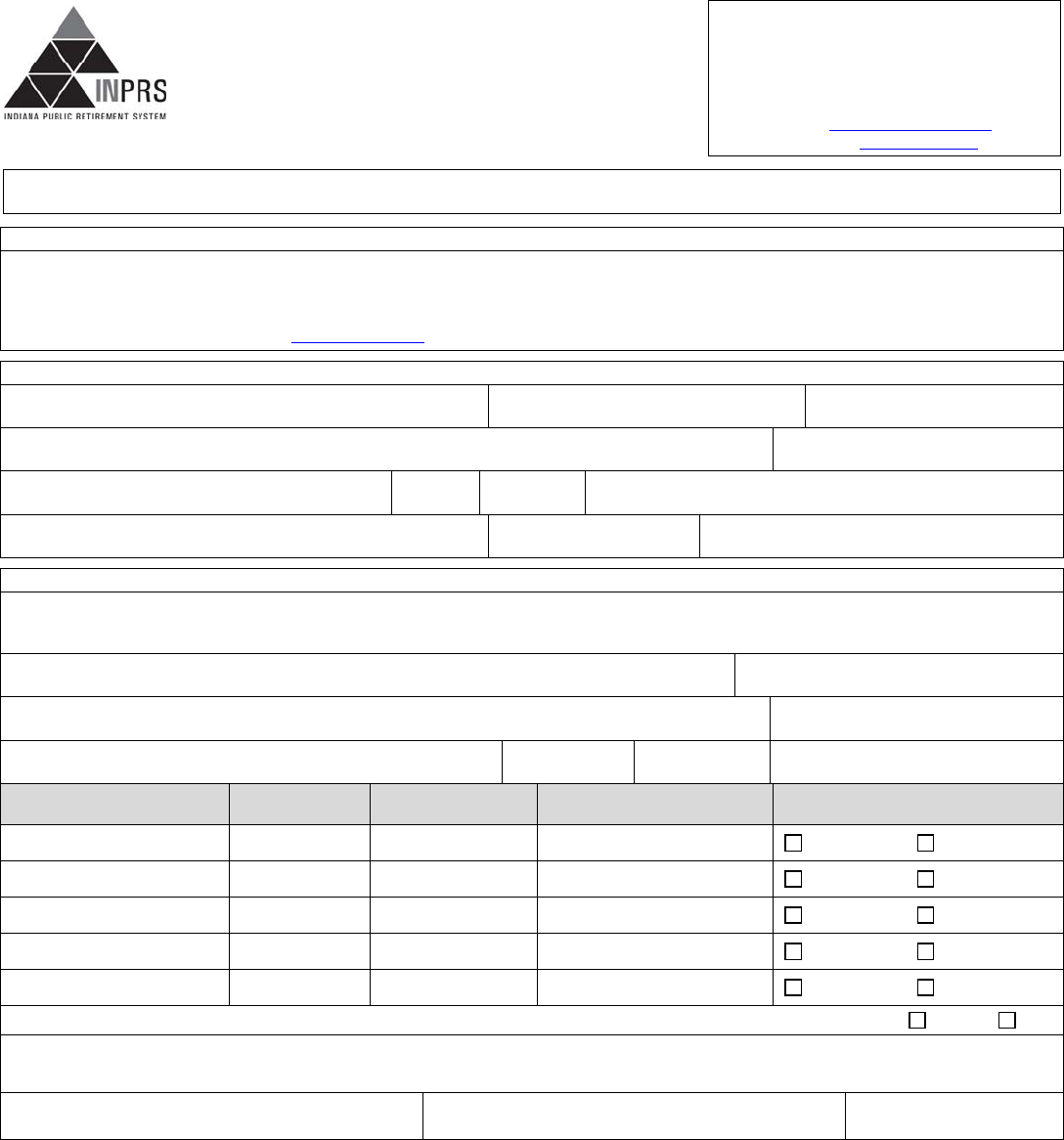
VERIFICATION OF PRIOR IN-STATE
TEACHING SERVICE
State Form 41625 (R7 / 2-13)
Approved by State Board of Accounts, 2013
INDIANA PUBLIC RETIREMENT SYSTEM
TEACHERS’ RETIREMENT FUND
1 North Capitol Avenue, Suite 001
Indianapolis, IN 46204-2014
Telephone: (888) 286-3544 (Toll-free)
Fax: (317) 232-3882
E-mail: [email protected]
Web site: www.inprs.in.gov
* This agency is requesting disclosure of Social Security Numbe rs in accordance w ith Internal Revenue Code 3405; disclosure is mandatory
and this form cannot be processed w ithout it.
INSTRUCTIONS
Member: Complete the MEMBER INFORMATION section and forward the form to the employer (school unit/corporation).
Employer: Complete the EMPLOYER AFFIDAVIT section and forward the form to the Indiana Public Retirement System (INPRS).
This information may be submitted by completing an adjusted wage and contribution transaction using TRF Employer Interactive
available on the INPRS Web site at www.inprs.in.gov
.
MEMBER INFORMATION
Member’s name
Social Security number (last 4 digits)*
Pension ID (PID) number
Address (number and street)
Telephone number with area code
City
State
ZIP Code
E-mail address
Member’s signature
Date (mm/dd/yyyy)
Maiden or other name used while teaching
EMPLOYER AFFIDAVIT
The member named in this form is seeking to verify teachin g service from your school district for the purpose of establishing
retirement credit in this Fund. Pursuant to Title 515 IAC 1, by signing this form, you, a representative of the emp loyer, are verifying
that this teacher was qualified to serve as a teacher and taught for the period of time indic ated on this form.
Employer/school corporation
Submission Unit number (if applicable)
Address (number and street)
Telephone number with area code
City
State
ZIP Code
Fax number with area code
School year taught
(July 1 through June 30)
Number of
days taught
Salary earned Position 3 percent Contribution paid by
$ Employer Employee
$ Employer Employee
$ Employer Employee
$ Employer Employee
$ Employer Employee
This service credit was in a public school covered under the Teachers’ Retirement Fund. Yes No
If any service occurred after July 1, 1995, this form will not be considered compl ete b y INPRS unless the employer has paid all
contributions in accordance with IC 5-10.4-7.
Authorized representativ e’s signature
Authorized representativ e’s title
Date (mm/dd/yyyy)
Reset Form
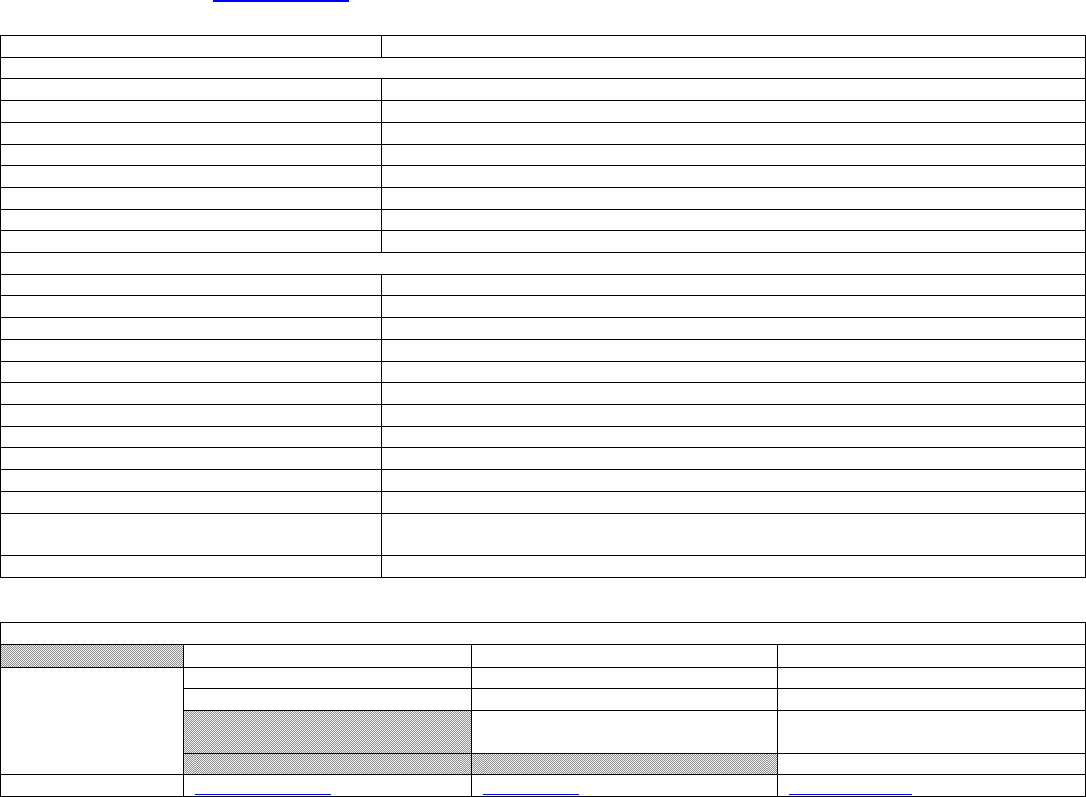
INSTRUCTIONS FOR
VERIFICATION OF IN-STATE TEACHING SERVICE
State Form 41625 (R7 / 2-13)
Page 1 of 1
IMPORTANT
Member: Complete the MEMBER INFORMATION section and forward the form to the employer (school unit/corporation).
Employer: Complete the EMPLOYER AFFIDAVIT section and forward the form to the Indiana Public Retirement S ystem (INPRS). This
information may be submitted by compl eting an adjusted wage and contri bution transaction using TRF Employer Interactive available
on the INPRS Web site at www.inprs.in.gov
.
1. Questions or changes? Call customer service, toll-free, at (888) 286-3544, Monday – Frid ay, 8 a.m.- 8 p.m. EST.
Entry field Field description
MEMBER INFORMATION
Member’s name Enter the member’s complete name.
Social Security number Enter the last 4 digits of the member’s Social Security number.
Pension ID (PID) number Enter the member’s Pension ID (PID) number.
Address, City, State, ZIP Code Enter the member’s street or mailing address.
Telephone number Enter the member’s telephone number including area code .
E-mail address Enter the member’s e-mail address, if applicable.
Maiden/Other name used while teaching Enter the member’s maiden or other name, if applicable.
Signature and date Sign and date the form; format = mm/dd/yyyy.
EMPLOYER
A
FFIDAVIT
School corporation’s name Enter the full name of the school corporation.
Submission unit number Enter the school’s submission unit number.
Address, City, State, ZIP Code Enter the school’s street or mailing address, city, state, and ZIP Code.
Telephone number Enter the school’s telephone number incl uding area code.
Fax number Enter the school’s fax number including area code.
School year taught Enter each year of teaching for the employee.
Number of days taught Enter the number of days taught for the year.
Salary earned Enter the employee’s salary earned for the year.
Position Enter the employee’s position for the year.
3 percent Contribution paid by Check either employer or employee as the payer of the mandator y 3% contribution.
Service credit Check Yes or No whether previous service was with TRF.
Authorized representat ive’s signature and
date
This form must be signed and dated b y the employer’s authorized representative.
Authorized representativ e’s printed title Enter the employer’s authorized representative’s title.
HELPFUL INFORMATION
INPRS/TRF INTERNAL REVENUE SERVICE
INDIANA DEPARTMENT OF REVENUE
Telephone
numbers
(888) 286-3544 Toll-free (800) 829-1040 Toll-free (317) 233-4018 Indianapolis local
Fax: (317) 232-3882 (800) 829-4477 TeleTax (317) 232-2240 Tax questio ns
(800) 829-4059 TDD (hearin g
impaired)
(317) 233-4952 TDD (hearin g
impaired)
(317) 233-2329 Fax
Web site
www.inprs.in.gov
www.irs.gov www.in.gov/dor


