
- Form DS-3 - Article 19-A Annual Affidavit of Compliance - New York
- Form DS-874C - Supplement to: Medical Examination of Driver Report - New York
- Form DS-19 - Motor Carrier Accident and Conviction Notification Program Application - New York
- Form IRP-21 - IRP TEAR Request Form - New York
- Form DS-872 - Carrier's Annual Review of Employee's Driving Record - New York
- Form DS-885 - Bus Driver Add/Drop Notice - New York
Fillable Printable Form DS-870 - Article 19-A Bus Driver Application - New York
Fillable Printable Form DS-870 - Article 19-A Bus Driver Application - New York
Form DS-870 - Article 19-A Bus Driver Application - New York
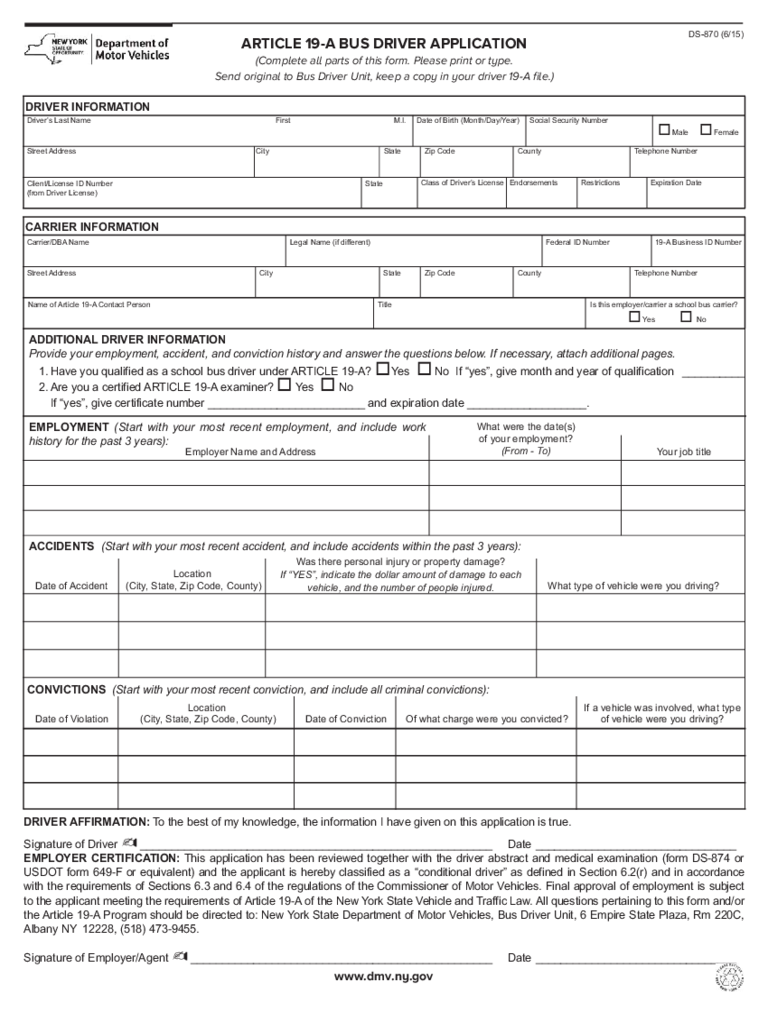
ARTICLE 19-A BUS DRIVER APPLICATION
(Complete all parts of this form. Please print or type.
Send original to Bus Driver Unit, keep a copy in your driver 19-A file.)
DRIVER AFFIRMATION: To the best of my knowledge, the information I have given on this application is true.
Signature of Driver
- ________________________________________________________ Date ________________________________
EMPLOYER CERTIFICATION: This application has been reviewed together with the driver abstract and medical examination (form DS-874 or
USDOT form 649-F or equivalent) and the applicant is hereby classified as a “conditional driver” as defined in Section 6.2(r) and in accordance
with the requirements of Sections 6.3 and 6.4 of the regulations of the Commissioner of Motor Vehicles. Final approval of employment is subject
to the applicant meeting the requirements of Article 19-A of the New York State Vehicle and Traffic Law. All questions pertaining to this form and/or
the Article 19-A Program should be directed to: New York State Department of Motor Vehicles, Bus Driver Unit, 6 Empire State Plaza, Rm 220C,
Albany NY 12228, (518) 473-9455.
DS-870 (6/15)
ADDITIONAL DRIVER INFORMATION
Provide your employment, accident, and conviction history and answer the questions below. If necessary, attach additional pages.
1. Have you qualified as a school bus driver under ARTICLE 19-A?
oYes o No If “yes”, give month and year of qualification __________
2. Are you a certified ARTICLE 19-A examiner?
o Yes o No
If “yes”, give certificate number _________________________ and expiration date ___________________.
EMPLOYMENT (Start with your most recent employment, and include work
history for the past 3 years):
ACCIDENTS (Start with your most recent accident, and include accidents within the past 3 years):
Employer Name and Address
What were the date(s)
of your employment?
(From - To)
Date of Accident
Location
(City, State, Zip Code, County)
Was there personal injury or property damage?
If “YES”, indicate the dollar amount of damage to each
vehicle, and the number of people injured.
What type of vehicle were you driving?
Your job title
CONVICTIONS (Start with your most recent conviction, and include all criminal convictions):
Date of Violation
Location
(City, State, Zip Code, County) Date of Conviction Of what charge were you convicted?
If a vehicle was involved, what type
of vehicle were you driving?
Signature of Employer/Agent - ________________________________________________ Date ________________________________
www.dmv.ny.gov
DRIVER INFORMATION
Driver’s Last Name
Street Address
Carrier/DBA Name Legal Name (if different)
Street Address City State Zip Code
19-A Business ID NumberFederal ID Number
City State Zip Code
Class of Driver’s License Endorsements Restrictions Expiration Date
Client/License ID Number
(from Driver License)
State
First M.I. Date of Birth (Month/Day/Year)
County Telephone Number
Social Security Number
oMale o Female
CARRIER INFORMATION
Name of Article 19-A Contact Person Title Is this employer/carrier a school bus carrier?
oYe s o No
County Telephone Number
reset/clear


