
Fillable Printable General Medicine Consult Form - Memphis
Fillable Printable General Medicine Consult Form - Memphis
General Medicine Consult Form - Memphis
Regional Medical Center at Memphis
INTERNAL MEDICINE CONSULT FORM
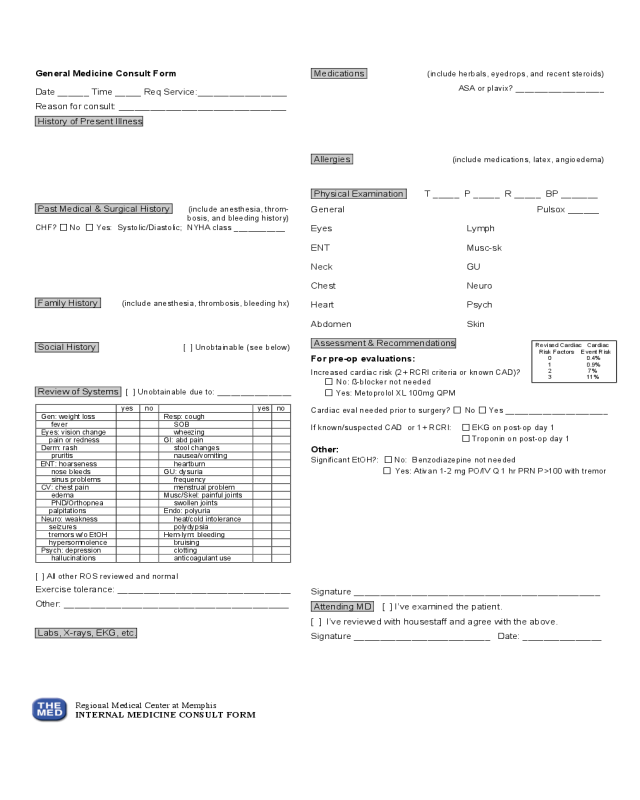
Revised Cardiac Cardiac
Risk Factors Event Risk
0 0.4%
1 0.9%
2 7%
3 11%
General Medicine Consult Form
Date ______ Time _____ Req Service:_________________
Reason for consult: ________________________________
History of Present Illness
Past Medical & Surgical History (include anesthesia, throm-
bosis, and bleeding history)
CHF? ⎔ No ⎔ Yes: Systolic/Diastolic; NYHA class ___________
Family History (include anesthesia, thrombosis, bleeding hx)
Social History [ ] Unobtainable (see below)
Review of Systems [ ] Unobtainable due to: ________________
[ ] All other ROS reviewed and normal
Exercise tolerance: _________________________________
Other: ___________________________________________
Labs, X-rays, EKG, etc.
Medications (include herbals, eyedrops, and recent steroids)
ASA or plavix? ___________________
Allergies (include medications, latex, angioedema)
Physical Examination T _____ P _____ R _____ BP _______
General Pulsox ______
Eyes Lymph
ENT Musc-sk
Neck GU
Chest Neuro
Heart Psych
Abdomen Skin
Assessment & Recommendations
For pre-op evaluations:
Increased cardiac risk (2+ RCRI criteria or known CAD)?
⎔ No: ß-blocker not needed
⎔ Yes: Metoprolol XL 100mg QPM
Cardiac eval needed prior to surgery? ⎔ No ⎔ Yes ______________________
If known/suspected CAD or 1+ RCRI: ⎔ EKG on post-op day 1
⎔ Troponin on post-op day 1
Other:
Significant EtOH?: ⎔ No: Benzodiazepine not needed
⎔ Yes: Ativan 1-2 mg PO/IV Q 1 hr PRN P>100 with tremor
Signature _______________________________________________
Attending MD [ ] I’ve examined the patient.
[ ] I’ve reviewed with housestaff and agree with the above.
Signature __________________________ Date: _______________
yes
no
yes
no
Gen: weight loss
Resp: cough
fever
SOB
Eyes: vision change
wheezing
pain or redness
GI: abd pain
Derm: rash
stool changes
pruritis
nausea/vomiting
ENT: hoarseness
heartburn
nose bleeds
GU: dysuria
sinus problems
frequency
CV: chest pain
menstrual problem
edema
Musc/Skel: painful joints
PND/Orthopnea
swollen joints
palpitations
Endo: polyuria
Neuro: weakness
heat/cold intolerance
seizures
polydypsia
tremors w/o EtOH
Hem-lym: bleeding
hypersomnolence
bruising
Psych: depression
clotting
hallucinations
anticoagulant use


