
Fillable Printable Injury and Illness Incident Report
Fillable Printable Injury and Illness Incident Report
Injury and Illness Incident Report
Information about the employee
Information about the physician or other health care
professional
Full name
Street
City State ZIP
Date of birth
Date hired
Male
Female
Name of physician or other health care professional
If treatment was given away from the worksite, where was it given?
Facility
Street
City State ZIP
Was employee treated in an emergency room?
Ye s
No
Was employee hospitalized overnight as an in-patient?
Ye s
No
_____________________________________________________________
________________________________________________________________
______________________________________ _________ ___________
______ / _____ / ______
______ / _____ / ______
__________________________
________________________________________________________________________
_________________________________________________________________
_______________________________________________________________
______________________________________ _________ ___________
r
r
r
r
r
r
U.S. Department of Labor
Occupational Safety and Health Administration
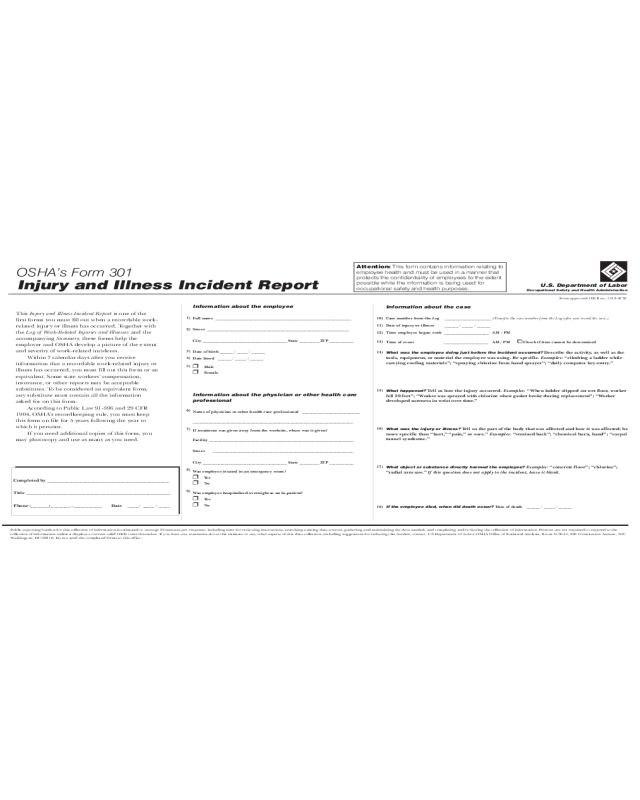
OSHA’s Form 301
Injury and Illness Incident Report
Form approved OMB no. 1218-0176
This is one of the
first forms you must fill out when a recordable work-
related injury or illness has occurred. Together with
the and the
accompanying these forms help the
employer and OSHA develop a picture of the extent
and severity of work-related incidents.
Within 7 calendar days after you receive
information that a recordable work-related injury or
illness has occurred, you must fill out this form or an
equivalent. Some state workers’ compensation,
insurance, or other reports may be acceptable
substitutes. To be considered an equivalent form,
any substitute must contain all the information
asked for on this form.
According to Public Law 91-596 and 29 CFR
1904, OSHA’s recordkeeping rule, you must keep
this form on file for 5 years following the year to
which it pertains.
If you need additional copies of this form, you
may photocopy and use as many as you need.
Injury and Illness Incident Report
Log of Work-Related Injuries and Illnesses
Summary,
Information about the case
Case number from the
Date of injury or illness
Time employee began work
Time of event Check if time cannot be determined
Date of death
Log _____________________ (Transfer the case number from the Log after you record the case.)
______ / _____ / ______
____________________
____________________
______ / _____ / ______
AM / PM
AM / PM
0
What was the employee doing just before the incident occurred?
What happened?
What was the injury or illness?
What object or substance directly harmed the employee?
If the employee died, when did death occur?
Describe the activity, as well as the
tools, equipment, or material the employee was using. Be specific. “climbing a ladder while
carrying roofing materials”; “spraying chlorine from hand sprayer”; “daily computer key-entry.”
Tell us how the injury occurred. “When ladder slipped on wet floor, worker
fell 20 feet”; “Worker was sprayed with chlorine when gasket broke during replacement”; “Worker
developed soreness in wrist over time.”
Tell us the part of the body that was affected and how it was affected; be
more specific than “hurt,” “pain,” or sore.” “strained back”; “chemical burn, hand”; “carpal
tunnel syndrome.”
“concrete floor”; “chlorine”;
“radial arm saw.”
Examples:
Examples:
Examples:
Examples:
If this question does not apply to the incident, leave it blank.
Completed by
Title
Phone Date
_______________________________________________________
_________________________________________________________________
(________)_________--_____________ _____/ ______ / _____
Public reporting burden for this collection of information is estimated to average 22 minutes per response, including time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. Persons are not required to respond to the
collection of information unless it displays a current valid OMB control number. If you have any comments about this estimate or any other aspects of this data collection, including suggestions for reducing this burden, contact: US Department of Labor, OSHA Office of Statistical Analysis, Room N-3644, 200 Constitution Avenue, NW,
Washington, DC 20210. Do not send the completed forms to this office.
10)
11)
12)
13)
14)
15)
16)
17)
18)
1)
2)
3)
5)
6)
7)
8)
9)
4)
Attention: This form contains information relating to
employee health and must be used in a manner that
protects the confidentiality of employees to the extent
possible while the information is being used for
occupational safety and health purposes.


