
Fillable Printable Letter of Medical Necessity Sample Form
Fillable Printable Letter of Medical Necessity Sample Form
Letter of Medical Necessity Sample Form
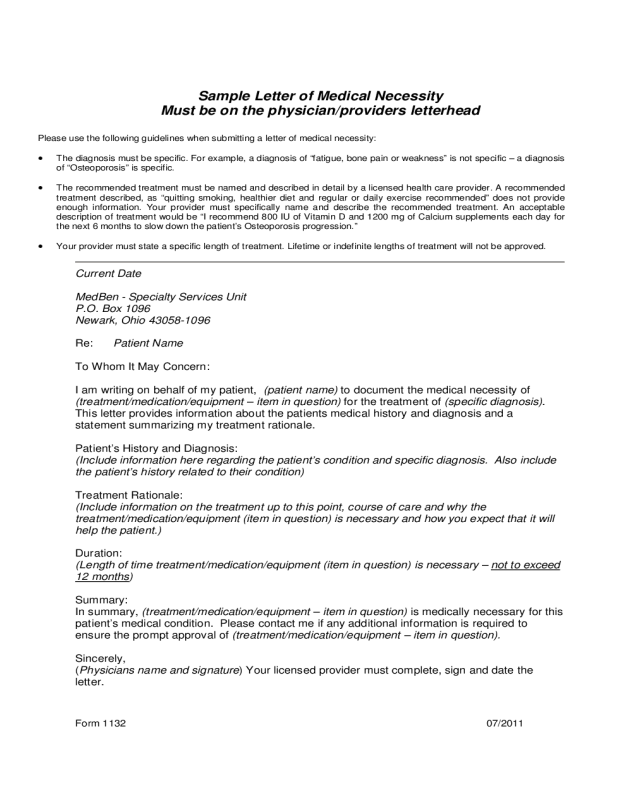
Sample Letter of Medical Necessity
Must be on the physician/providers letterhead
Form 1132 07/2011
Please use the following guid elines when submitting a l etter of medical n ecessit y:
• The diagnos is must be specific. F or example, a diagn osis of “f atigue, bone pain or weakness” is not specific – a diagn osis
of “Osteoporosis” is specific.
• The recommended treatment must be named and describe d in detail by a licensed health care provider . A recommended
treatment described, as “quitting smoking, healthier diet and regular or daily exercise recommended” does not provide
enough information. Your provider must specifically name and describe the recommended treatment. An acceptable
description of treatment would be “I recommend 800 IU of Vitamin D and 1200 mg of Calcium supplements each day for
the next 6 months to slow down the patient’s O steoporosis progression.”
• Your provider must state a specific length of treatment. Lifetime or indefinite lengths of treatment will not be approved.
Current Date
MedBen - Specialty Services Unit
P.O. Box 1096
Newark, Ohio 43058-1096
Re: Patient Name
To Whom It May Concern:
I am writing on behalf of my patient, (patient name) to document the medical necessity of
(treatment/medication/equipment – item in question) for the treatment of (specific diagnosis).
This letter provides information about the patients medical history and diagnosis and a
statement summarizing my treatment rationale.
Patient’s History and Diagnosis:
(Include information here regarding the patient’s condition and specific diagnosis. Also include
the patient’s history related to their condition)
Treatment Rationale:
(Include information on the treatment up to this point, course of care and why the
treatment/medication/equipment (item in question) is necessary and how you expect that it will
help the patient.)
Duration:
(Length of time treatment/medication/equipment (item in question) is necessary –
not to exceed
12 months)
Summary:
In summary, (treatment/medication/equipment – item in question) is medically necessary for this
patient’s medical condition. Please contact me if any additional information is required to
ensure the prompt approval of (treatment/medication/equipment – item in question).
Sincerely,
(Physicians name and signature) Your licensed provider must complete, sign and date the
letter.


