
Fillable Printable Mail Application for a Certified Copy of a Birth Certificate - Texas
Fillable Printable Mail Application for a Certified Copy of a Birth Certificate - Texas
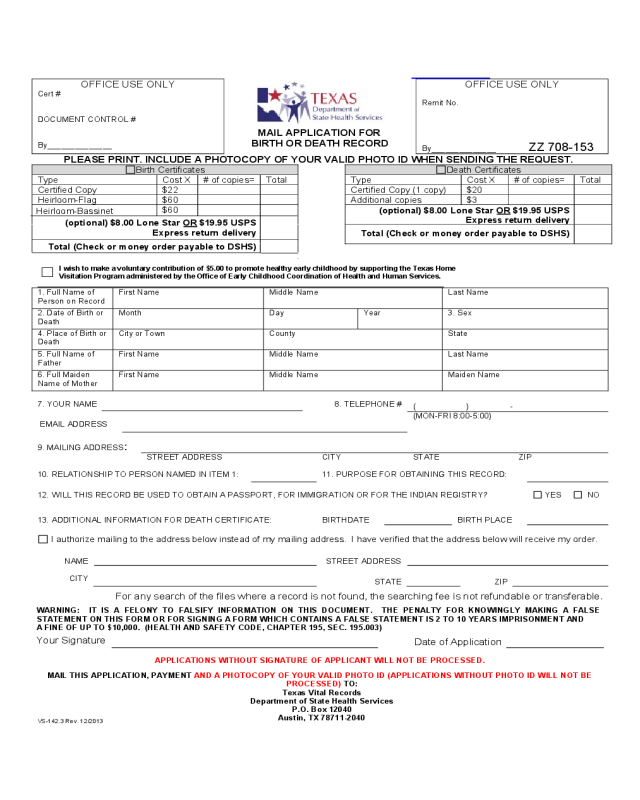
Mail Application for a Certified Copy of a Birth Certificate - Texas
OFFICE USE ONLY
Cert #
DOCUMENT CONTROL #
By______________
MAIL APPLICATION FOR
BIRTH OR DEATH RECORD
OFFICE USE ONLY
Remit No.
By______________
ZZ 708-153
PLEASE PRINT. INCLUDE A PHOTOCOPY OF YOUR VALID PHOTO ID WHEN SENDING THE REQUEST.
Birth Certificates Death Certificates
Type Cost X # of copies= Total Type Cost X # of copies= Total
Certified Copy $22 Certified Copy (1 copy) $20
Heirloom-Flag $60 Additional copies $3
Heirloom-Bassinet
$60
(optional) $8.00 Lone Star OR $19.95 USPS
Express return delivery
(optional) $8.00 Lone Star OR $19.95 USPS
Express return delivery
Total (Check or money order payable to DSHS)
Total (Check or money order payable to DSHS)
I wish to make a voluntary contribution of $5.00 to promote healthy early childhood by supporting the Texas Home
Visitation Program administered by the Office of Early Childhood Coordination of Health and Human Services.
1. Full Name of
Person on Record
First Name Middle Name Last Name
2. Date of Birth or
Death
Month Day Year 3. Sex
4. Place of Birth or
Death
City or Town County State
5. Full Name of
Father
First Name Middle Name Last Name
6. Full Maiden
Name of Mother
First Name Middle Name Maiden Name
7. YOUR NAME 8. TELEPHONE #
( ) -
EMAIL ADDRESS
(MON-FRI 8:00-5:00)
9. MAILING ADDRESS
:
STREET ADDRESS CITY STATE ZIP
10. RELATIONSHIP TO PERSON NAMED IN ITEM 1: 11. PURPOSE FOR OBTAINING THIS RECORD:
12. WILL THIS RECORD BE USED TO OBTAIN A PASSPORT, FOR IMMIGRATION OR FOR THE INDIAN REGISTRY? YES NO
13. ADDITIONAL INFORMATION FOR DEATH CERTIFICATE: BIRTHDATE
BIRTH PLACE
I authorize mailing to the address below instead of my mailing address. I have verified that the address below will receive my order.
NAME STREET ADDRESS
CIT
Y
STATE
ZIP
WARNING: IT IS A FELONY TO FALSIFY INFORMATION ON THIS DOCUMENT. THE PENALTY FOR KNOWINGLY MAKING A FALSE
STATEMENT ON THIS FORM OR FOR SIGNING A FORM WHICH CONTAINS A FALSE STATEMENT IS 2 TO 10 YEARS IMPRISONMENT AND
A FINE OF UP TO $10,000. (HEALTH AND SAFETY CODE, CHAPTER 195, SEC. 195.003)
Your Signature
Date of Application
APPLICATIONS WITHOUT SIGNATURE OF APPLICANT WILL NOT BE PROCESSED.
MAIL THIS APPLICATION, PAYMENT AND A PHOTOCOPY OF YOUR VALID PHOTO ID (APPLICATIONS WITHOUT PHOTO ID WILL NOT BE
PROCESSED) TO:
Texas Vital Records
Department of State Health Services
P.O. Box 12040
Austin, TX 78711-2040
VS-142.3 Rev. 12/2013
For any search of the files where a record is not found, the searching fee is not refundable or transferable.


