
Fillable Printable Medical Examination Report - California
Fillable Printable Medical Examination Report - California
Medical Examination Report - California
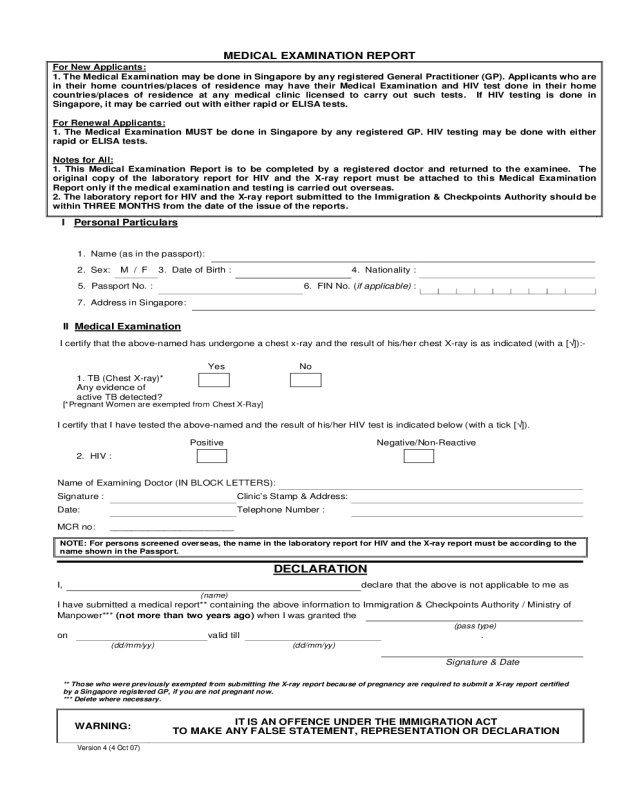
MEDICAL E XAMINATION REPORT
For New Applicants:
1. The Medical Examination may be done in Singapore by any registered General Practitioner (GP). Applicants who are
in their home countries/places of residence may have their Medical Examination and HIV test done in their home
countries/places of residence at any medical clinic licensed to carry out such tests. If HIV testing is done in
Singapore, it may be carried out w ith either rapid or ELISA tests.
For Renewal Applicants:
1. The Medical Examination MUST be done in Singapore by any registered GP. HIV testing may be done with either
rapid or ELISA tests.
Notes for All:
1. This Medical Examination Report is to be completed by a registered doctor and returned to the examinee. The
original copy of the laboratory report for HIV and the X-ray report must be attached to this Medical Examination
Report only if the medical examination and testing is carried out overseas.
2. The laboratory report for HIV and the X-ray report submitted to the Immigration & Checkpoints Authority should be
w ithin THREE MONTHS from the d ate o f the issue of the reports.
I Personal Particulars
1. Name (as in the passport):
2. Sex: M / F 3. Date of Birth : 4. Nationality :
5. Passport No. : 6. FIN No. (if applicable) :
7. Address in Singapore:
II Medical Examination
I certify that the above-named has un dergone a chest x-ra y and the result of his/her ches t X-ray is as indicated (with a [√]):-
Yes No
1. TB (Chest X-ray)*
Any evidence of
active TB detected?
[*Pregnant Women are exempted from Chest X-Ray]
I certify that I have tested the above-named and the result of his/her HIV test is indicated below (with a tick [√]).
Positive Negative/Non-Reactive
2. HIV :
Name of Examinin g Doctor (IN BLOCK LETTERS):
Signature : Clinic’s Stamp & Address:
Date: Telephone Number :
MCR no: _______________ ________
NOTE: For persons screened overseas, the name in the laboratory report for HIV and the X-ray report must be accordi ng to the
name shown in the Passport.
DECLARATION
I, declare that the abov e is not applicable to me as
(
name
)
I have submitted a medical re port** containing the above information to Immigration & Checkpoints Authority / Ministry of
Manpow er*** (n ot more than two years ago) when I was granted the
(p
ass t
yp
e
)
on valid till .
(dd/mm/yy) (dd/mm/yy)
Signature & Date
** Those who were previously exempted from submitting the X-ray report because of pregnancy are required to submit a X-ray report certified
by a Singapore register ed GP, if you are not pregnant now.
*** Delete where necessary.
WARNING:
IT IS AN OFFENCE UNDER THE IMMIGRATION ACT
TO MAKE ANY FALSE STATEMENT, REPRESENTATION OR DECLARATION
Version 4 (4 Oct 07)


