
Fillable Printable Medical Examner's Certificate
Fillable Printable Medical Examner's Certificate
Medical Examner's Certificate
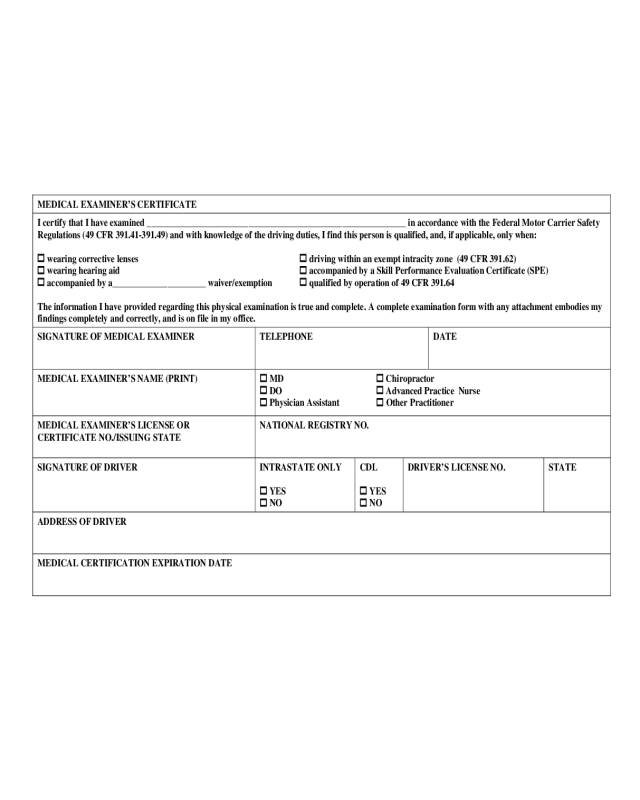
MEDICAL EXAMINER’S CERTIFICATE
I certify that I have examined _____________________________________________________________ in ac cordan ce wit h the Federal Motor Carrier Safety
Regulat ions (49 CFR 391.41-391.49) and with knowledge of the driving duties, I find this person is qualified, and, if applicable, onl y whe n:
wearing corrective lenses
driving within an exempt intracity zone (49 CF R 391.62)
wearing hearing aid
accom panied by a Skill Performance Evalu ation C erti ficate (SPE)
ac com pani ed by a______________________ waiver/exemption
qualified by operation of 49 CFR 391.64
The information I have provided regarding this physical examination is true and complete. A complete examination form with any attachment embodies my
findings completely and correctly, and is on file in my office.
SIGNATURE OF MEDICAL EXAMINER
TELEPHONE
DATE
MEDICAL EXAMINER’S NAME (PRINT)
MD Chiropractor
DO
Advanced Practice Nurse
Physician Assistant
Other Practitioner
MEDICAL EXAMINER’S LICENSE OR
CERTIFICATE NO./ISSUING STATE
NATIONAL REGISTRY NO.
SIGNATURE OF DRIVER
INTRASTATE ONLY
YES
NO
CDL
YES
NO
DRIVER’S LICENSE NO.
STATE
ADDRESS OF DRIVER
MEDICAL CERTIFICATION EXPIRATION DATE


