
Fillable Printable Motor Insurance Claim Form
Fillable Printable Motor Insurance Claim Form
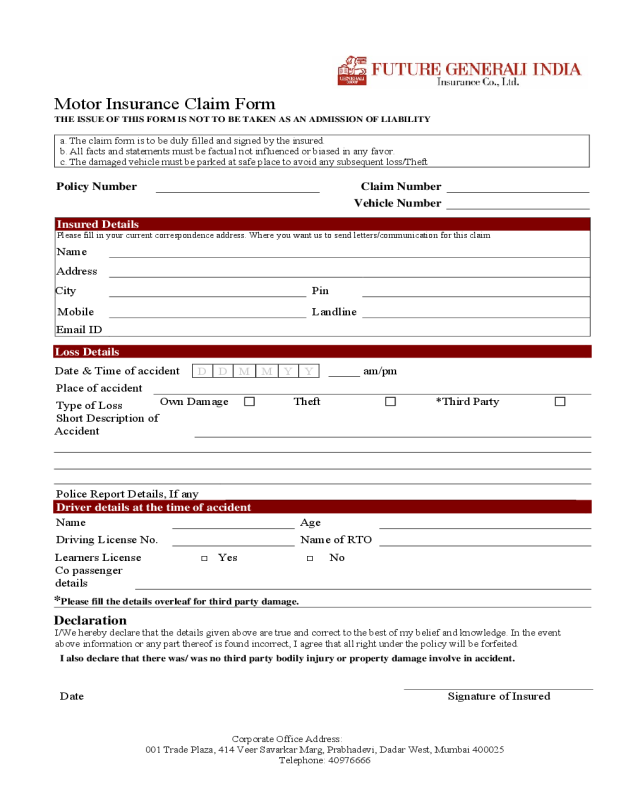
Motor Insurance Claim Form
a. The claim form is to be duly filled and signed by the insured.
b. All facts and statements must be factual not influenced or biased in any favor.
c. The damaged vehicle must be parked at safe place to avoid any subsequent loss/Theft
Policy Number
Claim Number
Vehicle Number
Insured Details
Please fill in your current correspondence address. Where you want us to send letters/communication for this claim
Name
Address
City Pin
Mobile Landline
Email ID
Loss Details
Date & Time of accident _____ am/pm
D D M M Y Y
Place of accident
Type of Loss
Own Damage Theft *Third Party
Short Description of
Accident
Police Report Details, If any
___________________________________________________________________
Driver details at the time of accident
Name Age
Driving License No. Name of RTO
Learners License □ Yes □ No
Co passenger
details
*Please fill the details overleaf for third party damage.
Declaration
I/We hereby declare that the details given above are true and correct to the best of my belief and knowledge. In the event
above information or any part thereof is found incorrect, I agree that all right under the policy will be forfeited.
I also declare that there was/ was no third party bodily injury or property damage involve in accident.
Date Signature of Insured
Motor Insurance Claim Form
THE ISSUE OF THIS FORM IS NOT TO BE TAKEN AS AN ADMISSION OF LIABILIT Y
Corporate Office Address:
001 Trade Plaza, 414 Veer Savarkar Marg, Prabhadevi, Dadar West, Mumbai 400025
Telephone: 40976666
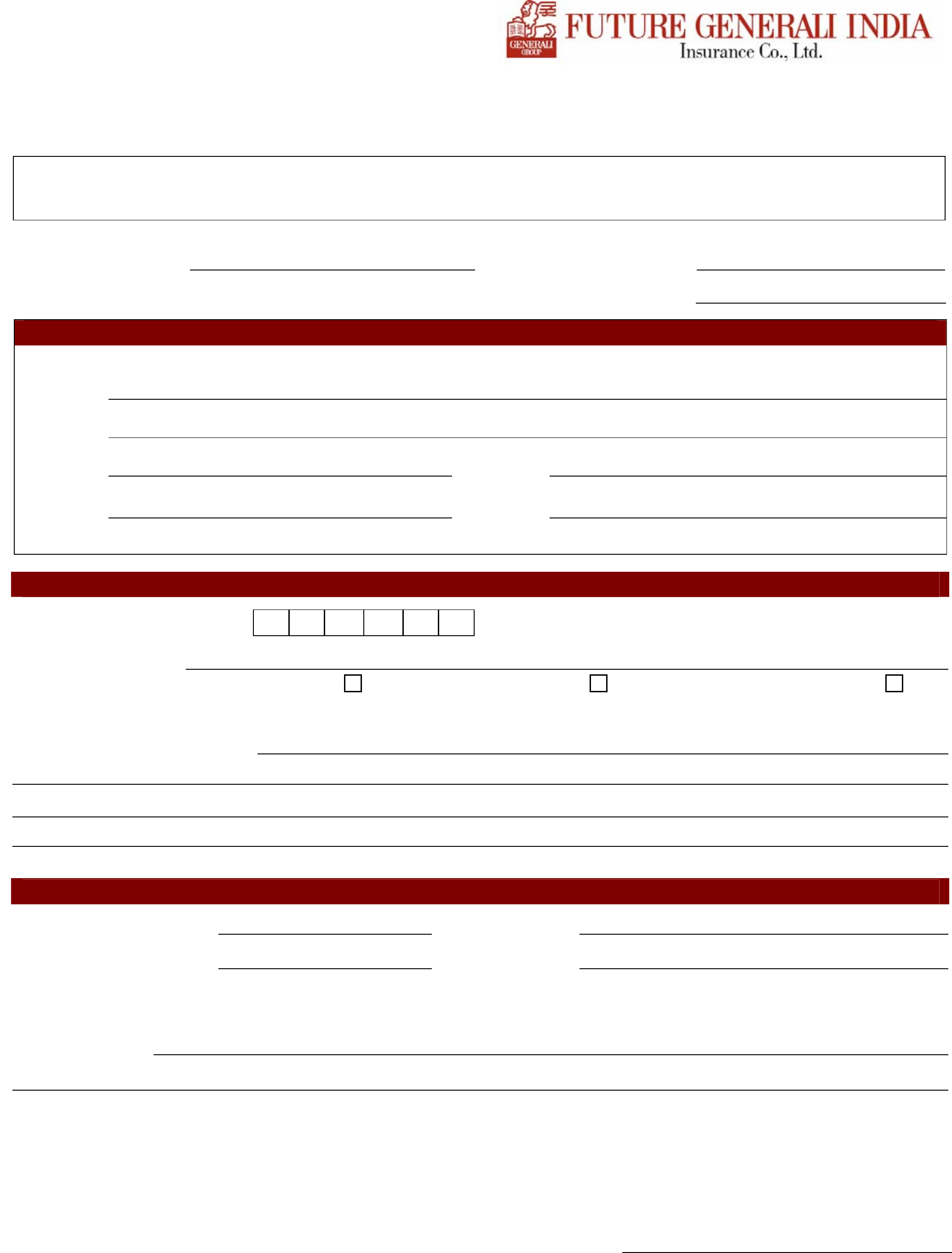
Applicable for commercial vehicle:
No. of Passenger carried at the time of
accident G R Number & Date
Permit No Permit Issuing Authority
Permit Valid up to Permit valid for (Area)
Applicable for third party property damage or injury
Name of Third
Party/Occupants
/Driver
Contact No
Fitness Granting Authority Fitness valid up to
Type of Injury Name of the Hospital
where admitted
Any Legal/
Court Notice
Received
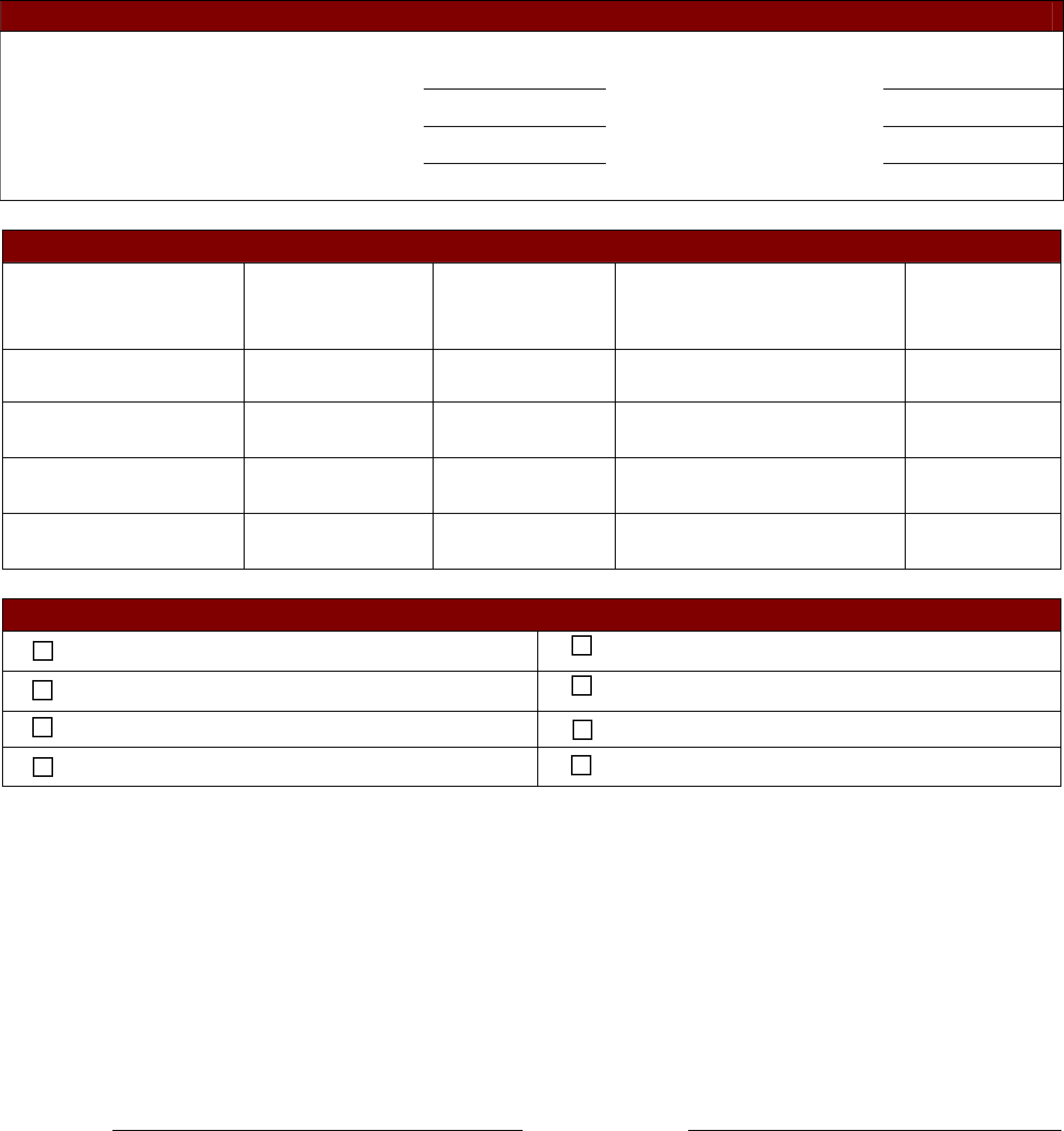
I hereby declare having submitted the following documents:
Copy of Policy/Cover Note Copy of Fitness Certificate
Copy of RC Book Copy of Permit
Copy of Driving License Copy of FIR
Estimate of Repairs G.R Form
DECLARATION
I/We here by declare that the details given above are true and correct to the best of my belief and
knowledge .In event above information or nay part thereof is found incorrect, I agree that all rights
under the policy will be fortified. I/We also agree to provide additional information to the company,
if required.
Date Signature of Insured
Corporate Office Address:
001 Trade Plaza, 414 Veer Savarkar Marg, Prabhadevi, Dadar West, Mumbai 400025
Telephone: 40976666


