
Fillable Printable My Medicine Record - Department of Health and Human Services
Fillable Printable My Medicine Record - Department of Health and Human Services
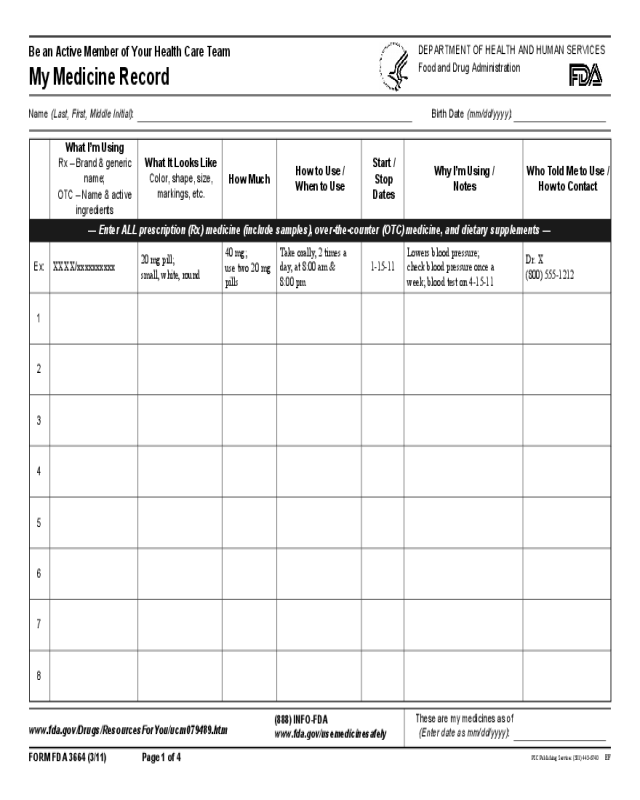
My Medicine Record - Department of Health and Human Services
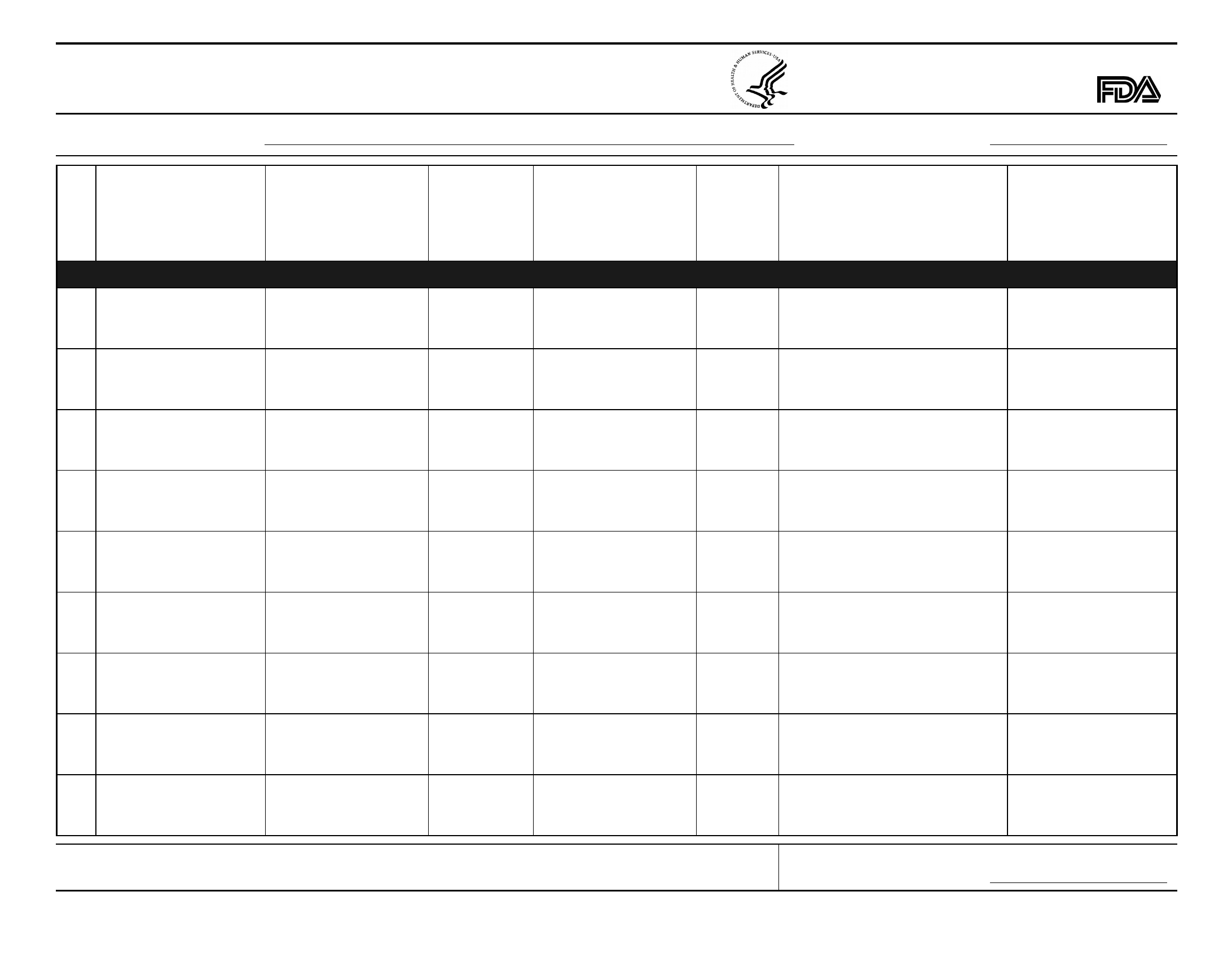
What I’m Using
Rx – Brand & generic
name;
OTC – Name & active
ingredients
What It Looks Like
Color, shape, size,
markings, etc.
How Much
How to Use /
When to Use
Start /
Stop
Dates
Why I’m Using /
Notes
Who Told Me to Use /
How to Contact
— Enter ALL prescription (Rx) medicine (include samples), over-the-counter (OTC) medicine, and dietary supplements —
Ex:
XXXX/xxxxxxxxxx
20 mg pill;
small, white, round
40 mg;
use two 20 mg
pills
Take orally, 2 times a
day, at 8:00 am &
8:00 pm
1-15-11
Lowers blood pressure;
check blood pressure once a
week; blood test on 4-15-11
Dr. X
(800) 555-1212
1
2
3
4
5
6
7
8
DEPARTMENT OF HEALTH AND HUMAN SERVICES
Food and Drug Administration
Be an Active Member of Your Health Care Team
My Medicine Record
Name (Last, First, Middle Initial):
www.fda.gov/Drugs/ResourcesForYou/ucm079489.htm
Birth Date (mm/dd/yyyy):
These are my medicines as of
(Enter date as mm/dd/yyyy):
(888) INFO-FDA
www.fda.gov/usemedicinesafely
FORM FDA 3664 (3/11) Page 1 of 4
PSC Publishing Services (301) 443-6740
EF
FORM FDA 3664 (3/11) Page 2 of 4
www.fda.gov/Drugs/ResourcesForYou/ucm079489.htm (888) INFO-FDA
www.fda.gov/usemedicinesafely
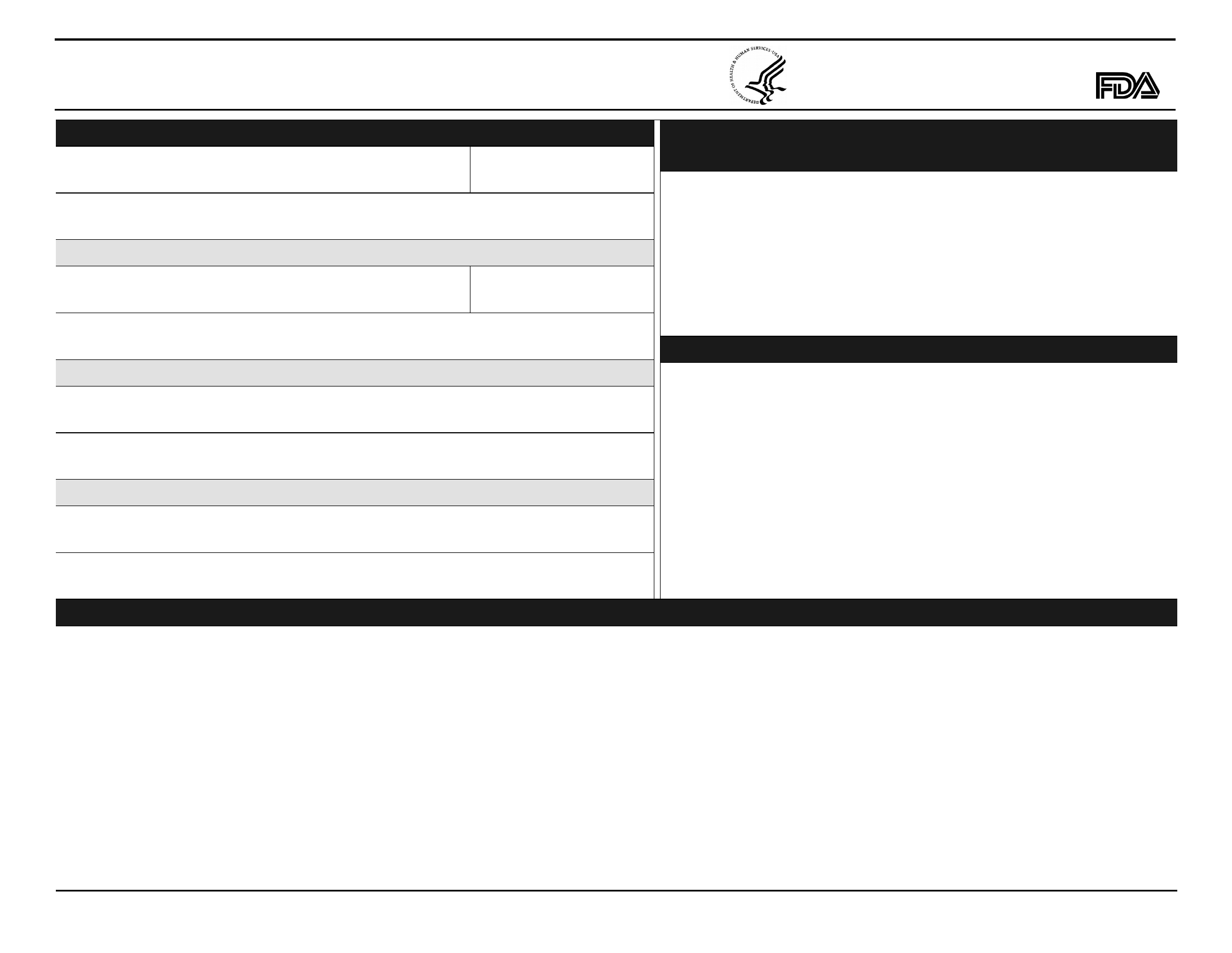
My Personal Contacts
Questions I Should Ask About Medicines or Dietary Supplements
Allergic Reaction or Other Problem I’ve Had With…
any medicine, dietary supplement, food, skin cleaner, medical tape
My Medical Conditions and Operations
Emergency Contact
Primary Care Physician
Pharmacy / Drugstore
My Name (Last, First, Middle Initial)
Fill in the record for any new medicine, prescription (Rx) or
over-the-counter (OTC), or dietary supplement, or ask my
doctor or pharmacist to help me fill it in. Make sure I can read
what is written on the record.
When I review the record, or a change is made, ask:
• Can I use a generic form?
• When should I start to feel differently? When should I report back
to the doctor?
• Will this take the place of anything else I am using?
• Are there any special directions for using this?
Name
Name
Name
Contact Information
Contact Information
Contact Information
Contact Information
Birth Date (mm/dd/yyyy)
Relationship
Describe in space below.
Describe in space below.
• Should I avoid any other medicines, dietary supplements, or
treatments while using this?
• Should I avoid any drinks, foods, other substances, or activities
while using this?
• What are the possible side effects from this? Is there anything I
should watch for? What do I do if I get a side effect?
• Will I need any tests (blood tests, x-rays, other) to make sure it is
working as it should? When? How will I get the results?
• What should I do if I miss a dose? What do I do if I use too much?
• Where and how can I get more written information about this?
DEPARTMENT OF HEALTH AND HUMAN SERVICES
Food and Drug Administration
My Medicine Record
Be an Active Member of Your Health Care Team
FORM FDA 3664 (3/11) Page 3 of 4
www.fda.gov/Drugs/ResourcesForYou/ucm079489.htm
(888) INFO-FDA
www.fda.gov/usemedicinesafely
•
Use this record with the “Be An Active Member of Your Health
Care Team” pamphlet, found at:
www.fda.gov/Drugs/ResourcesForYou/UCM079529#pamphlet
•
Save “My Medicine Record” on your personal computer (PC).
Type information into the fields with your keyboard. You can also
print the record and enter the information with a pencil.
•
Enter ALL prescription medicines you use, including
any medicine samples you are given.
•
Enter ALL over-the-counter medicines and dietary
supplements (including vitamins, minerals, and herbals) you
use, whether you use them all the time or only some of the time.
•
Print and share the record with your doctors, pharmacists, or
other health professionals at ALL your visits.
•
Keep a printed copy with you all the time. It is a good idea to
give a copy to a friend or loved one.
Review this record and update it on your PC or by hand when
you:
• Stop or start a medicine or dietary supplement
• Make a change in anything you use
• Visit your doctor, pharmacist, or other health professional
What I’m Using
•
Prescription (Rx) medicine – enter the brand and generic name
of the medicine, including any samples you are given
•
Over-the-Counter (OTC) medicine – enter the name and active
ingredient(s), including OTCs you use for allergies, stomach
ache, heartburn, nausea; OTC pain relievers you use for minor
aches and pains, headache, fever; OTC cold medicines,
laxatives, sleeping pills, and others prescribed by your doctor,
such as aspirin
• Dietary supplements, including vitamins, minerals, and herbals
What it Looks Like
• Form (pill, tablet, capsule, liquid, injection, suppository, cream,
lotion, eye or ear drops, etc.)
• Shape, color, size, and scoring (any lines on the medicine) or
other markings
How Much
• Dose that you are directed to use either by the doctor or pharmacist
or by the directions on the label
• If you are to use a dose which is different than the dose the
medicine comes in, note the number you use (for example, you
are supposed to use 40 mg, and it comes in 20 mg pills, put “40
mg; use two 20 mg pills” or “2 pills”)
How to Use / When to Use
•
How to use – such as “swallow with water; do not chew” or “take
by mouth with food” or “two times a day”)
•
When to use – the time, or time of day, you use it (such as
“10:00 pm” or “at bedtime”)
Start / Stop Dates
• Date you started using it. If you are only supposed to use it for a
period of time, put the date you should stop using it
• If it is something you use sometimes, such as an OTC you use
only when you have a headache, put “when needed”
How to Use My Medicine Record
DEPARTMENT OF HEALTH AND HUMAN SERVICES
Food and Drug Administration
Be an Active Member of Your Health Care Team
My Medicine Record
FORM FDA 3664 (3/11) Page 4 of 4
www.fda.gov/Drugs/ResourcesForYou/ucm079489.htm
(888) INFO-FDA
www.fda.gov/usemedicinesafely
Why I’m Using / Notes
• The reason why you are using it, such as “high blood pressure”
• Any special directions on how to use the medicine, such as
whether to take it with or without food
• Any tests that are needed to find out it is working as it should,
and dates you need the tests
• How and where to keep or store it, if not at room temperature
Who Told Me to Use / How to Contact
• Name and contact information of the doctor, nurse, or pharmacist
(or other) who prescribed or told you to use it
My Personal Contacts
• Contact information for you, someone you want contacted in an
emergency, your doctor, pharmacy, or pharmacist. Under “Contact
Information,” enter phone number or e-mail address. An extra
space is there for an extra contact person, if needed.
Allergic Reaction or Other Problem I’ve Had With...
• Any medicine, dietary supplement, food, skin cleaner, medical
tape with which you have had a problem
• Also enter anything that could have an effect on your use, such
as pregnancy, breast feeding, trouble swallowing tablets, or
trouble remembering to use. Include problems with ingredients,
such as colors, flavors, starches, or sugars.
My Medical Conditions and Operations
• Any diseases, illnesses, or medical conditions, such as asthma,
diabetes, heart disease, high blood pressure, kidney disease, or
cancer
• Any conditions or problems you often treat with prescription or
over-the-counter medicine or dietary supplements, such as acid
stomach or allergies
• Operations you’ve had
Questions I Should Ask About Medicines or Dietary Supplements
• Fill in the record for any new medicine or dietary supplement, or
ask your doctor or pharmacist to help you fill it in. Make sure you
can read what is written. If you can’t read it, others may have
trouble reading it, too. Use these questions when you review the
record with your health professionals or when a change is made
in something you use.
How to Use My Medicine Record
DEPARTMENT OF HEALTH AND HUMAN SERVICES
Food and Drug Administration
Be an Active Member of Your Health Care Team
My Medicine Record


