
Fillable Printable Obstetrical Pre-admission Registration - Cape Fear Valley Health System
Fillable Printable Obstetrical Pre-admission Registration - Cape Fear Valley Health System
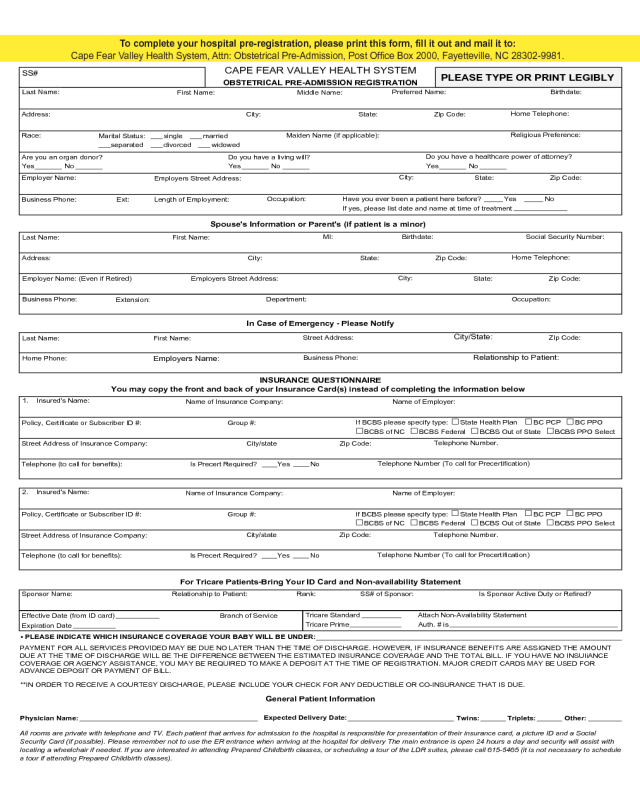
Obstetrical Pre-admission Registration - Cape Fear Valley Health System
Is Precert Required? Yes No
Do you have a healthcare power of attorney?
Yes No
Do you have a living will?
Yes No
Are you an organ donor?
Yes No
Marital Status: single married
separated divorced widowed
CAPE FEAR VALLEY HEALTH SYSTEM
SS#
PLEASE TYPE OR PRINT LEGIBLY
OBSTETRICAL PRE-ADMISSION REGISTRATION
Spouse's Information or Parent's (if patient is a minor)
In Case of Emergency - Please Notify
INSURANCE QUESTIONNAIRE
You may copy the front and back of your Insurance Card(s) instead of completing the information below
For Tricare Patients-Bring Your ID Card and Non-availability Statement
Rank: SS# of Sponsor: Is Sponsor Active Duty or Refired?Sponsor Name: Relationship to Patient:
Tricare Standard Attach Non-Availability Statement
Branch of Service
Effective Date (from ID card)
Tricare Prime Auth. # is
Expiration Date
• PLEASE INDICATE WHICH INSURANCE COVERAGE YOUR BABY WILL BE UNDER:
PAYMENT FOR ALL SERVICES PROVIDED MAY BE DUE NO LATER THAN THE TIME OF DISCHARGE. HOWEVER, IF INSURANCE BENEFITS ARE ASSIGNED THE AMOUNT
DUE AT THE TIME OF DISCHARGE WILL BE THE DIFFERENCE BETWEEN THE ESTIMATED INSURANCE COVERAGE AND THE TOTAL BILL. IF YOU HAVE NO INSUIiANCE
COVERAGE OR AGENCY ASSISTANCE, YOU MAY BE REQUIRED TO MAKE A DEPOSIT AT THE TIME OF REGISTRATION. MAJOR CREDIT CARDS MAY BE USED FOR
ADVANCE DEPOSIT OR PAYMENT OF BILL.
**IN ORDER TO RECEIVE A COURTESY DISCHARGE, PLEASE INCLUDE YOUR CHECK FOR ANY DEDUCTIBLE OR CO-INSURANCE THAT IS DUE.
Expected Delivery Date:
Twins:Physician Name: Other:
Triplets:
All rooms are private with telephone and TV. Each patient that arrives for admission to the hospital is responsible for presentation of their insurance card, a picture ID and a Social
Security Card (if possible). Please remember not to use the ER entrance when arriving at the hospital for delivery The main entrance is open 24 hours a day and security will assist with
locating a wheelchair if needed. If you are interested in attending Prepared Childbirth classes, or scheduling a tour of the LDR suites, please call 615-5465 (it is not necessary to schedule
a tour if attending Prepared Childbirth classes).
Lost Name:
First Name:
Middle Name:
Preferred Name: Birthdate:
Home Telephone:
Address: State: Zip Code:
City:
Maiden Name (if applicable):
Religious Preference:
Race:
State:
Employer Name:
City:
Zip Code:
Employers Street Address:
Business Phone:
Ext:
Occupation:
Length of Employment:
Have you ever been a patient here before? Yes No
If yes, please list date and name at time of treatment
MI:
Birthdate: Social Security Number:
Last Name:
First Name:
Home Telephone:
State: Zip Code:
Address: City:
City:
State: Zip Code:
Employers Street Address:
Employer Name: (Even if Retired)
Department:
Business Phone: Occupation:
Extension:
Name of Employer:
Name of Insurance Company:
Policy, Certificate or Subscriber ID #: Group #:
Telephone Number.
Zip Code:
City/state
Street Address of Insurance Company:
Telephone Number (To call for Precertification)
Telephone (to call for benefits):
City/State:
ZIp Code:
Street Address:
Last Name:
First Name:
Business Phone:
Relationship to Patient:
Home Phone:
Employers Name:
1. Insured's Name:
If BCBS please specify type: State Health Plan BC PCP BC PPO
BCBS of NC BCBS Federal BCBS Out of State BCBS PPO Select
Is Precert Required? Yes No
Name of Employer:
Name of Insurance Company:
Policy, Certificate or Subscriber ID #: Group #:
Telephone Number.
Zip Code:
City/state
Street Address of Insurance Company:
Telephone Number (To call for Precertification)
Telephone (to call for benefits):
2. Insured's Name:
If BCBS please specify type: State Health Plan BC PCP BC PPO
BCBS of NC BCBS Federal BCBS Out of State BCBS PPO Select
General Patient Information
Last Name:
To complete your hospital pre-registration, please print this form, ll it out and mail it to:
Cape Fear Valley Health System, Attn: Obstetrical Pre-Admission, Post Ofce Box 2000, Fayetteville, NC 28302-9981.


