
Fillable Printable Patient Feedback Form Sample
Fillable Printable Patient Feedback Form Sample
Patient Feedback Form Sample
Please ask your next three existing patients to complete this form
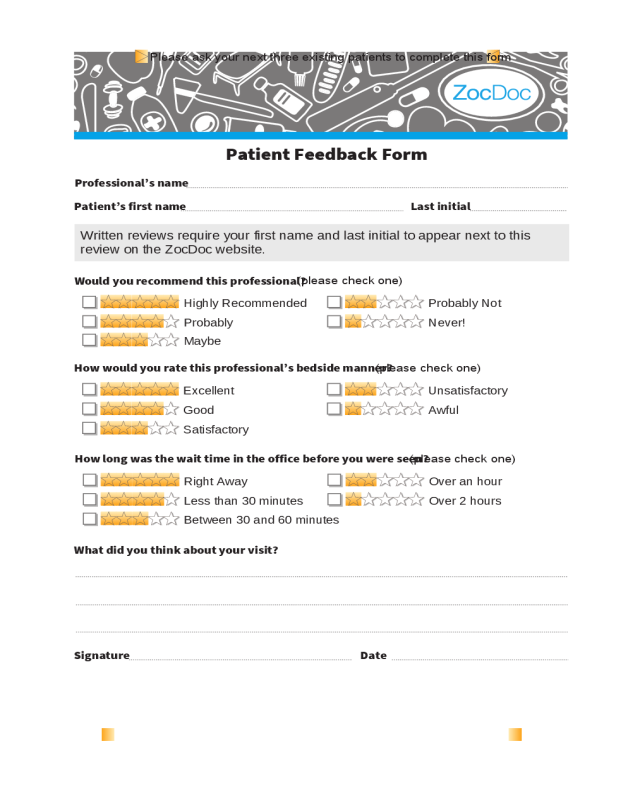
Patient Feedback Form
Professional’s name
Patient’s first name Last initial
Signature Date
Written reviews require your first name and last initial to appear next to this
review on the ZocDoc website.
Would you recommend this professional?
(please check one)
Highly Recommended Probably Not
Probably Never!
Maybe
How would you rate this professional’s bedside manner?
(please check one)
Excellent Unsatisfactory
Good Awful
Satisfactory
How long was the wait time in the office before you were seen?
(please check one)
What did you think about your visit?
Right Away Over an hour
Less than 30 minutes Over 2 hours
Between 30 and 60 minutes


