
Fillable Printable Pension Withdrawal Form - New Jersey
Fillable Printable Pension Withdrawal Form - New Jersey
Pension Withdrawal Form - New Jersey

CW-0493-0702
STATE OF NEW JERSEY
DIVISION OF PENSIONS AND BENEFITS
Public Employees' Retirement System
Teachers' Pension and Annuity Fund
Police and Firemen's Retirement System
State Police Retirement System
APPLICATION FOR WITHDRAWAL
PO Box 295
Trenton, NJ 08625-0295

FREQUENTLY ASKED QUESTIONS
1. Who is eligible to withdraw?
To withdraw the balance of your pension contributions
in a lump sum, you must have resigned your position
and no longer be employed in a covered position.
Withdrawal is not permitted by law if you are on a leave
of absence granted by your employer.
An employee who is receiving periodic Workers’ Com-
pensation benefits as the result of an injury incurred in
public employment is considered an active employee
and an active member of the pension fund. If you are
receiving Workers’ Compensation benefits, or have a
case pending, applying for withdrawal from the pension
fund could jeopardize your rights to benefits. In such
cases, the Division will require that you complete an
additional retirement benefit waiver form.
If you were dismissed from your position and are in the
process of appealing that dismissal, you cannot with-
draw your contributions until a decision has been ren-
dered or your appeal is withdrawn.
If you hold more than one position covered under the
pension fund (multiple membership), you cannot with-
draw until you have terminated all employment covered
by the pension fund.
2. What is inactive membership?
When you resign your position, you may leave your
contributions on deposit and continue an inactive mem-
bership in the fund for a maximum period of two years.
Should you return to active service in a position cov-
ered by the pension fund before the expiration of your
membership, you may reactivate your account with the
same service credit established at the time you ceased
employment.
The period during which you were inactive will not
count as service credit for retirement.
If your position was abolished due to a layoff, your
employer must notify the Division of Pensions and Ben-
efits in writing, and your membership in the fund can
remain inactive for a maximum of ten years (five years
for PFRS members).
3. How do I apply for withdrawal?
You must complete Part One and Part Two of the Appli-
cation for Withdrawal. Be sure to sign and date your
application.
Your former employer is responsible for the Employer‘s
Certification for Withdrawal form. Your withdrawal claim
cannot be paid until your former employer has complet-
ed this form.
If you are a member of the New Jersey State Employ-
ees Deferred Compensation Plan or Supplemental
Annuity Collective Trust (SACT), you must file separate
applications for withdrawal from those plans. You can
obtain an application by calling the Deferred Compen-
sation Plan at (609) 292-3605, or SACT at (609) 633-
2031.
4. What happens to my Group Life Insurance when I
withdraw?
Group Life Insurance coverage will expire 31 days after
your termination of employment. You may convert all or
any part of your insurance to an individual policy by
contacting the Prudential Insurance Company of Amer-
ica, Inc. at 1-800-262-1112.
Contributions made for Contributory Group Life Insur-
ance are not refundable upon termination of employ-
ment.
5. If I am taking another job in New Jersey govern-
ment, must I withdraw?
If you are terminating employment to accept another
position covered by any government agency in New
Jersey (except federal government), you may transfer
your account. Please call the Office of Client Services
at (609) 292-7524 for more information.
6. I have 10 years of service credit, but have not
reached normal retirement age. Must I withdraw?
If you have established at least 10 years of service
credit and have not reached normal retirement age, you
can apply for Deferred Retirement, whereby you begin
collecting a monthly pension at the normal retirement
age. Call the Benefits Information Library at (609) 777-
1931 and request catalog item 210 for information
about Deferred Retirement.
Normal retirement age for the Public Employees'
Retirement System (PERS) and the Teachers' Pension
and Annuity Fund (TPAF) is 60. Normal retirement age
for the Police and Firemen's Retirement System
(PFRS) or the State Police Retirement System (SPRS)
is 55.
You are not eligible for Deferred Retirement if you with-
draw your contributions.
7. What is payable when I withdraw?
If you terminate employment or cease to be an employ-
ee for any reason other than death or retirement, you
shall receive all of the accumulated deductions stand-
ing to your credit in your individual account less any
outstanding loan balance.
Withdrawing members of the PERS or TPAF who have
at least three years of contributing membership service
at the time the service ceases will have interest credit-
ed.
No interest is payable to withdrawing members of the
PFRS or SPRS.
CW-0493-0201q
1
DO NOT RETURN THE APPLICATION WITHOUT COMPLETING PART TWO.
2
INSTRUCTIONS FOR COMPLETING THE WITHDRAWAL APPLICATION
PART ONE AND PART TWO OF THE APPLICATION FOR WITHDRAWAL are to be complet-
ed by the member and signed. The application should then be returned to the Division of
Pensions and Benefits. If you have difficulty completing this form, please call the Division
of Pensions and Benefits, Office of Client Services at (609) 292-7524 for assistance. The
Division of Pensions and Benefits cannot give tax advice.
P
ART ONE:
ITEM 2 — ADDRESS
Withdrawal checks must be mailed. They cannot be picked up at the Division of Pensions
and Benefits. If you move between the time you file the application and the check is
mailed, you may change your address by contacting the Division’s Office of Client Ser-
vices at (609) 292-7524.
ITEMS 5 and 6 — RETIREMENT SYSTEM/MEMBER NUMBER
Be sure to indicate your retirement system and membership number. If you are not sure,
consult your personnel, payroll office, or look on your annual Personal Benefits Statement.
ITEM 9 — REASON FOR TERMINATION
You must indicate the reason and date of your termination. See Question #1 of the Fre-
quently Asked Questions for information on dismissal.
ITEM 10 — WORKERS’ COMPENSATION CASES
If you are receiving Workers’ Compensation benefits, the Division is required to send
you an additional retirement benefit waiver form which you must complete and return
before we can process your withdrawal.
ITEM 11 — WAIVER OF RETIREMENT BENEFITS
Please read the instructions on the application and the information in Question #6 of the
Frequently Asked Questions carefully before completing this waiver. If you have 10 years
of membership credit or are age 58 or older (PERS and TPAF) and do not complete this
item, you will be required to complete and return a separate benefit waiver form before we
can process your withdrawal.
P
ART TWO: ROLLOVER ELECTION — SELECTION OF PAYMENT TYPE
If Part Two is not completed or completed incorrectly, the Division of Pensions and Benefits will
make your total payment payable to you and withhold 20% federal income tax on the taxable por-
tion of your payment.
Please carefully read the payment selection information on the following page, the instructions
on the application, and Fact Sheet #27 — The Taxability and Mandatory Withholding of Income
Tax from your Pension Distribution before completing this portion of your application. Your selec-
tion in Part Two of the application can not be changed once your application has been processed.
Call the Automated Information System at (609) 777-1777 to hear your approximate taxable
amount and other information concerning withdrawal.
(
continued on next page)
(PART TWO continued from previous page)
Selection 1 - If you choose this selection, the Division of Pensions and Benefits will make your
benefit check payable to you at the address listed in Part 1. 20% of the taxable portion
of your payment will be withheld as federal income tax.
Selection 2 - If you choose this selection, there will be a direct rollover of the entire taxable
and non-taxable portion of your payment. This selection is onl
y open to those
whose taxable portion is $200 or more. You must insert the name of the financial insti-
tution or employer plan that will accept your rollover. The Division of Pensions and Bene-
fits will mail a check to you which will be made payable to the institution or employer plan
you selected to accept your rollover.
Selection 3 - If you choose this selection, there will be a direct rollover of the entire taxable
portion of your payment. This selection is onl
y open to those whose taxab
le portion
is $200 or more
.
You must insert the name of the financial institution or employer plan
that will accept your rollover. The Division of Pensions and Benefits will mail a check to
you representing the taxable portion of your payment which will be made payable to the
institution or employer plan you selected to accept your rollover. If part of your payment
is non-taxable, a second check for the non-taxable portion will be made payable to you.
Selection 4 - If you choose this selection, there will be a direct rollover of part of the taxable
portion of your payment. This selection is onl
y open to those whose taxable portion
is $200 or more. You must insert the dollar amount you wish to roll over and the name
of the financial institution or employer plan that will accept your rollover. Any remaining
portion of your taxable amount will be paid to you in a separate check, less 20% for fed-
eral tax, along with any non-taxable amount.
Selection 5 - If you choose this selection, there will be a direct rollover of the entire taxable
portion of your payment, along with a portion of your non-taxable payment. This
selection is only open to those whose taxable portion is $200 or more. You must
insert the dollar amount of the non-taxable portion that you wish to roll over and the name
of the financial institution or employer plan that will accept your rollover. The remaining
portion of your non-taxable amount will be paid to you in a separate check.
P
ART THREE: SIGNATURE
Be sure to sign and date your application. For your own protection, unsigned applications
will not be processed. The Division cannot accept photocopies or facsimiles of complet-
ed applications.
NOTE: If you are a participant in the Supplemental Annuity Collective Trust (SACT) or New
Jersey State Employees Deferred Compensation Plan (NJSEDCP), and are with-
drawing all accumulated salary deductions in the retirement system, a separate applica-
tion to withdraw from these plans must be filed and submitted to the Division of Pensions
and Benefits. To obtain an application please call (609) 633-2031 for SACT or (609) 292-
3605 for NJSEDCP.
EMPLO
YER CERTIFICATION
The Employer Certification for Withdrawal form must be filled out by your former
employer after you have terminated employment. While the employer’s certifi-
cation does not have to accompany your Application for Withdrawal, WE CAN-
NOT PROCESS YOUR APPLICATION UNTIL WE RECEIVE THE EMPLOYER'S CER-
TIFICATION.
3
CW-0493-0702
State of New Jersey — Department of the Treasury
Division of Pensions and Benefits, PO Box 295, Trenton, NJ 08625-0295 — (609) 292-7524
APPLICATION FOR WITHDRAWAL
Please read instructions carefully before completing the application.
PART ONE: To be completed by member. Please print.
1. Name _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
FIRST MIDDLE INITIAL LAST
2. Mailing Address _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
STREET APT. NO.
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
CITY STATE ZIP CODE
3. Daytime Telephone No. (__________) _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
AREA CODE
4. D a t e o f B i r t h _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
MONTH DAY YEAR
5. I am a member of (check one only):
Public Employees’ Retirement System
Teachers’ Pension and Annuity Fund
Police and Firemen’s Retirement System
State Police Retirement System
6. Member No. _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
7. Social Security No. _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
8. Employer _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
9. Please indicate the reason and date you terminated employment Resigned Dismissed
Date: _______/_______/_______
MONTH, DAY, YEAR
10. I AM, or AM NOT receiving periodic benefits under a claim filed for Workers’ Compensation based on an
injury incurred as a result of service performed in public employment.
I DO, or DO NOT have a Workers’ Compensation claim or litigation pending.
11. Members having 10 or more years of membership credit or who are within 2 years of normal retirement age must
waive any monthly retirement benefits by completing the waiver below. This item must be completed before
your application can be processed. If you do not complete the waiver, you will receive an estimate of the retire-
ment and group life insurance benefits for which you would be eligible and a benefit waiver form which must be
completed and returned before we can process your withdrawal. Any member who is at least age 60 (for PERS
and TPAF) or at least age 55 (for PFRS and SPRS) will automatically receive an estimate of retirement
benefits and waiver form to complete.
Although I am eligible for retirement, I elect to withdraw my pension contributions and hereby waive my
right to receive a lifetime monthly allowance and group life insurance at retirement in favor of receiving a
refund of my pension contributions now.
______________________________________________
(You must sign here)
PLEASE COMPLETE SIDE 2
Member’s Name ________________________________________________ Member No. _____________________
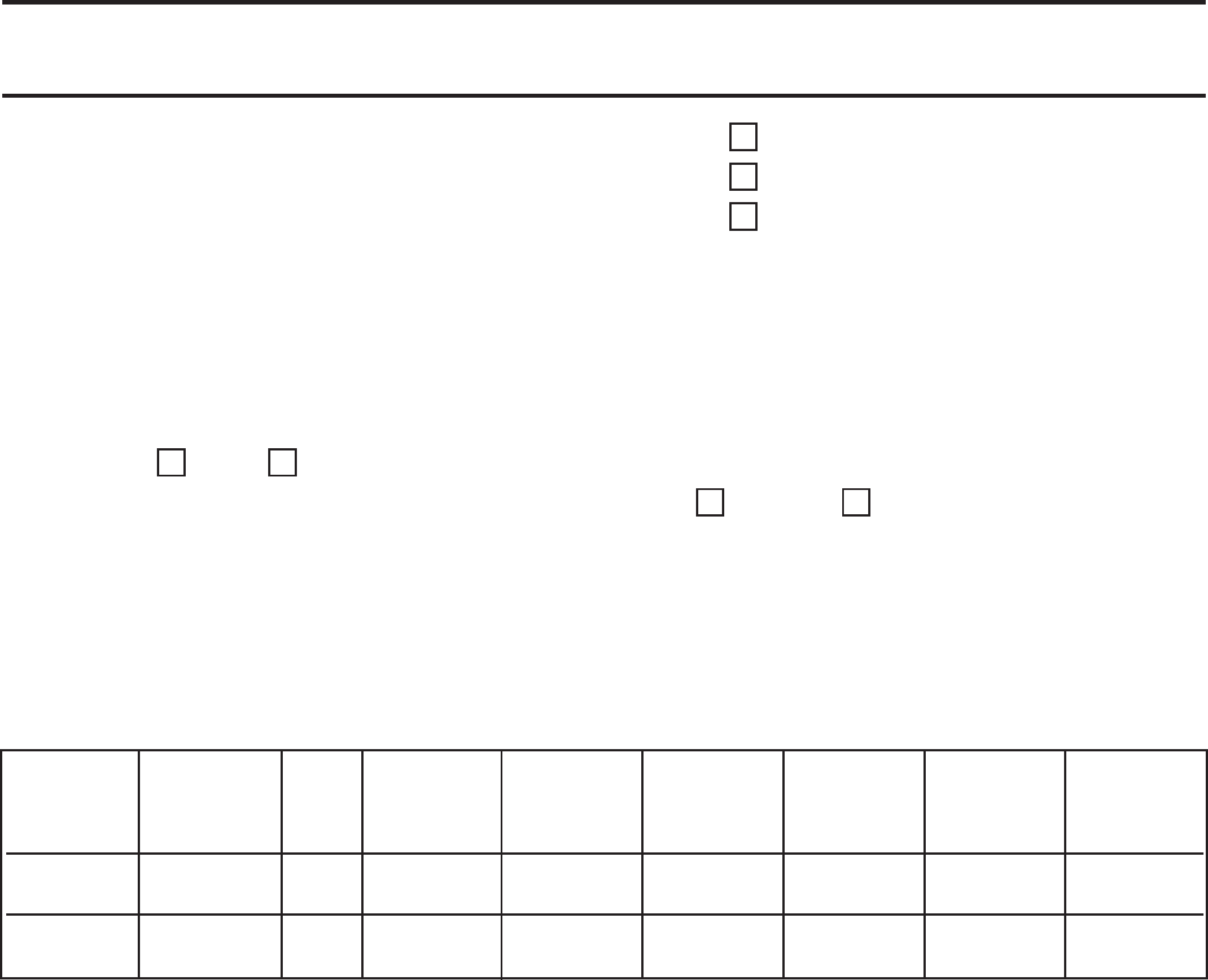
PART TWO: To be completed by member. Please print
.
Please carefully read the following section and indicate your choice by checking one of the boxes below
(this selection is irrevocable once made). For an explanation of these selections read the instructions for
Part Two in Completing the Withdrawal Application. If P
art Two is not completed or is completed incor-
rectly, the Division of Pensions and Benefits will automatically withhold 20% federal income tax.
Call the
Automated Information System at (609) 777-1777 to hear your approximate taxable amount and other infor-
mation concerning withdrawal.
IMPORTANT: YOUR SELECTION IS IRREVOCABLE.
Rollover is only available if the taxable portion of your payment is $200 or more.
1. Withhold 20% federal income tax on the taxable portion of my payment.
2. Roll over the entire payment including any after tax contributions to:
Print the name of the financial
institution or employer plan ___________________________________________________________________
This is an: IRA Employer Plan
3. Roll over the entire taxab
le portion of my payment to:
Print the name of the financial
institution or employer plan ___________________________________________________________________
This is an: IRA Employer Plan
4. Roll over $_______________ (dollar amount) of the taxable portion of my payment to:
Print the name of the financial
institution or employer plan ___________________________________________________________________
This is an: IRA Employer Plan
5. Roll over the entire taxable portion and $_______________ (dollar amount) of the non-taxable portion of
my payment to:
Print the name of the financial
institution or employer plan ___________________________________________________________________
This is an: IRA Employer Plan
PART 3: I have read both the letter and fact sheet sent with this form. I understand that the Division of Pensions and Ben-
efits will act upon my choice in Part Two. I under
stand my selection in Part Two cannot be changed.
_______________________________________________________________ ____________________________
Signature Date
CW-0493-0702
CW-0493-0702
State of New Jersey — Department of the Treasury
Division of Pensions and Benefits, PO Box 295, Trenton, NJ 08625-0295 — (609) 292-7524
EMPLOYER’S CERTIFICATION FOR WITHDRAWAL
THIS FORM MUST BE COMPLETED BY FORMER EMPLOYER
1. Name of Member __________________________________________________________________________
2. Membership No. __________________________ 3. Social Security No. __________________________
This certification will be used to calculate the payment due to the member.
DO NOT COMPLETE THIS FORM UNTIL THE LAST DEDUCTION FROM SALARY HAS BEEN MADE.
resigned
I certify that _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ was dismissed (no appeal pending)
NAME OF FORMER EMPLOYEE
was dismissed (appeal pending)
from this organization on __________________. The last pension deduction was made _______________________________.
DATE BIWEEKLY PAY PERIOD / YEAR OR
MONTH/ YEAR*
*State employers must enter the number of the pay period and the year of the last pension deduction.
All other employers must enter the month and year of the last pension deduction and be sure to sub-
mit that deduction for the entire month.
The employee IS, or IS NOT receiving periodic benefits under a claim filed for Workers’ Compensation based on an
injury incurred as a result of service performed in public employment and DOES, or DOES NOT have a Workers’ Com-
pensation claim or litigation pending.
CERTIFICATION OF SALARY DEDUCTIONS
ONLY TO BE COMPLETED FOR ANY UNPOSTED PENSION CONTRIBUTIONS
I certify that the following deductions have been made from the employee's salary during the last two quarterly periods ending
with the current quarter. State biweekly reporting agencies must attach a completed Supplemental Biweekly Certification of
Employing Agency or a screen print of the Centralized Payroll History screen in lieu of completing this item.
Signature of
Certifying Officer _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Date _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Employing Agency _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Telephone Number _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
(INCLUDE AREA CODE)
BASE SALARY
SUBJECT TO FULL ARREARS TOTAL
QUARTER CONTRIBUTIONS RATE PENSION LOAN BACK AND/OR PENSION SACT
ENDING THIS QUARTER (%) CONTRIBUTION REPAYMENT DEDUCTIONS PURCHASES CONTRIBUTIONS YES OR NO
$$$$$$
$$$$$$
INSTRUCTIONS FOR COMPLETING THE EMPLOYER’S CERTIFICATION
This certification must be completed by the employer when a member files an
application for withdrawal of pension contributions. Failure to provide this
information will delay processing of the member's application for withdrawal.
If you need assistance in completing this certification, call the Division of Pen-
sions and Benefits’ Office of Client Services at (609) 292-7524 weekdays
between 9:00 a.m. and 4 p.m. (except State holidays).
ITEMS REQUIRING SPECIAL
ATTENTION
REASON FOR LEAVING
You must indicate the member’s reason for leaving. Place an (X) the box next to “resigned,” or if the member was
dismissed, you must also indicate with an (X) if the dismissal has an appeal pending or no appeal pending. This infor-
mation is required before processing the withdrawal application.
TERMINATION DATE
A member must terminate employment before this certification can be submitted to the Division of Pensions and
Benefits. Include the date of termination and the date of the last pension deduction. State biweekly reporting agen-
cies must enter the number and year of the last pay period of the last pension deduction. All other employ-
ers must enter the month and year of the last pension deduction.
WORKER’S COMPENSATION
Please indicate if the member was receiving periodic benefits under a claim filed for Worker’s Compensation. Place
an (X) in the block to indicate if the member IS or IS NOT receiving these benefits. You must also indicate with an
(X) if the member DOES or DOES NOT have a Worker’s Compensation claim or litigation pending. This information
is required before processing the withdrawal application.
SALARY DEDUCTIONS
Indicate the following: (1) quarter ending, (2) amount of monthly base salary subject to contributions, (3) full rate of
contribution, (4) the dollar amount of the deduction, (5) loan repayment amount (if any), (6) back deductions, (7)
arrears or purchase deductions, (8) the total pension contributions (include all deductions for the quarter), and (9)
answer “yes” or “no” to whether the member contributed to the Supplemental Annuity Collective Trust (SACT).
SUBMIT THIS CERTIFICATION TO: WITHDRAWAL SECTION
DIVISION OF PENSIONS AND BENEFITS
PO BOX 295
TRENTON NJ 08625-0295


