
Fillable Printable Physical Therapy Evaluation Form Sample
Fillable Printable Physical Therapy Evaluation Form Sample
Physical Therapy Evaluation Form Sample
PHYSICAL THERAPY INITIAL EVALUATION FORM
PATIENT INFORMATION DATE_____________________
NAME_______________________________________________ OCCUPATION______________________________________________
(LAST) (FIRST)
BIRTHDATE_______________________ AGE______ HEIGHT____________ WEIGHT________lbs
HOME/CELL PHONE___________________________________ EMPLOYER________________________________________________
CURRENTLY EMPLOYED? YES NO MODIFIED
REHAB INFORMATION
1. CHIEF COMPLAINT/AILMENT/INJURY_____________________________________________________________________________
2. DATE OF INJURY__________________________ DATE OF SURGERY_______________________
3. BRIEFLY DESCRIBE HOW YOU WERE INJURED
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
4. HAVE YOU RECEIVED THERAPY FOR THIS CONDITION? YES NO WHEN?_______________________
HOW MANY VISITS?____________
5. HAS YOUR CONDITION BEEN GETTING: WORSE SAME BETTER
6. ARE YOUR SYMPTOMS: CONSTANT OR INTERMITTENT
7. MARK THE NUMBER THAT BEST CORRESPONDS TO YOUR PAIN:
AT BEST: 0 1 2 3 4 5 6 7 8 9 10 (EXCRUCIATING PAIN)
AT WORST: 0 1 2 3 4 5 6 7 8 9 10 (EXCRUCIATING PAIN)
8. WHAT DECREASES/MAKES YOUR CONDITION BETTER? (MARK ALL THAT APPLY)
BENDING MOVEMENT REST BETTER IN AM
SITTING STANDING HEAT BETTER AS DAY PROGRESSES
RISING WALKING ICE BETTER IN PM
CHANGING POSITIONS LYING MEDICATION N/A CAST JUST REMOVED
9. WHAT INCREASES/MAKES YOUR CONDITION WORSE? (MARK ALL THAT APPLY)
BENDING MOVEMENT REST SNEEZE
SITTING STANDING STAIRS DEEP BREATH
RISING WALKING COUGH MEDICATION
PROLONGED POSITIONING LYING WORSE IN AM WORSE IN PM
WORSE AS DAY PROGRESSES N/A CAST JUST REMOVED
10. PREVIOUS MEDICAL INTERVENTION (MARK ALL THAT APPLY)
X-RAY MRI CATSCAN INJECTIONS OTHER______________________________________________________
Patient#_______________ Provider_______
11. WHAT ARE YOUR GOALS TO BE ACHIEVED BY THE END OF THERAPY?
________________________________________________________________________________________________________________
________________________________________________________________________________________________________________
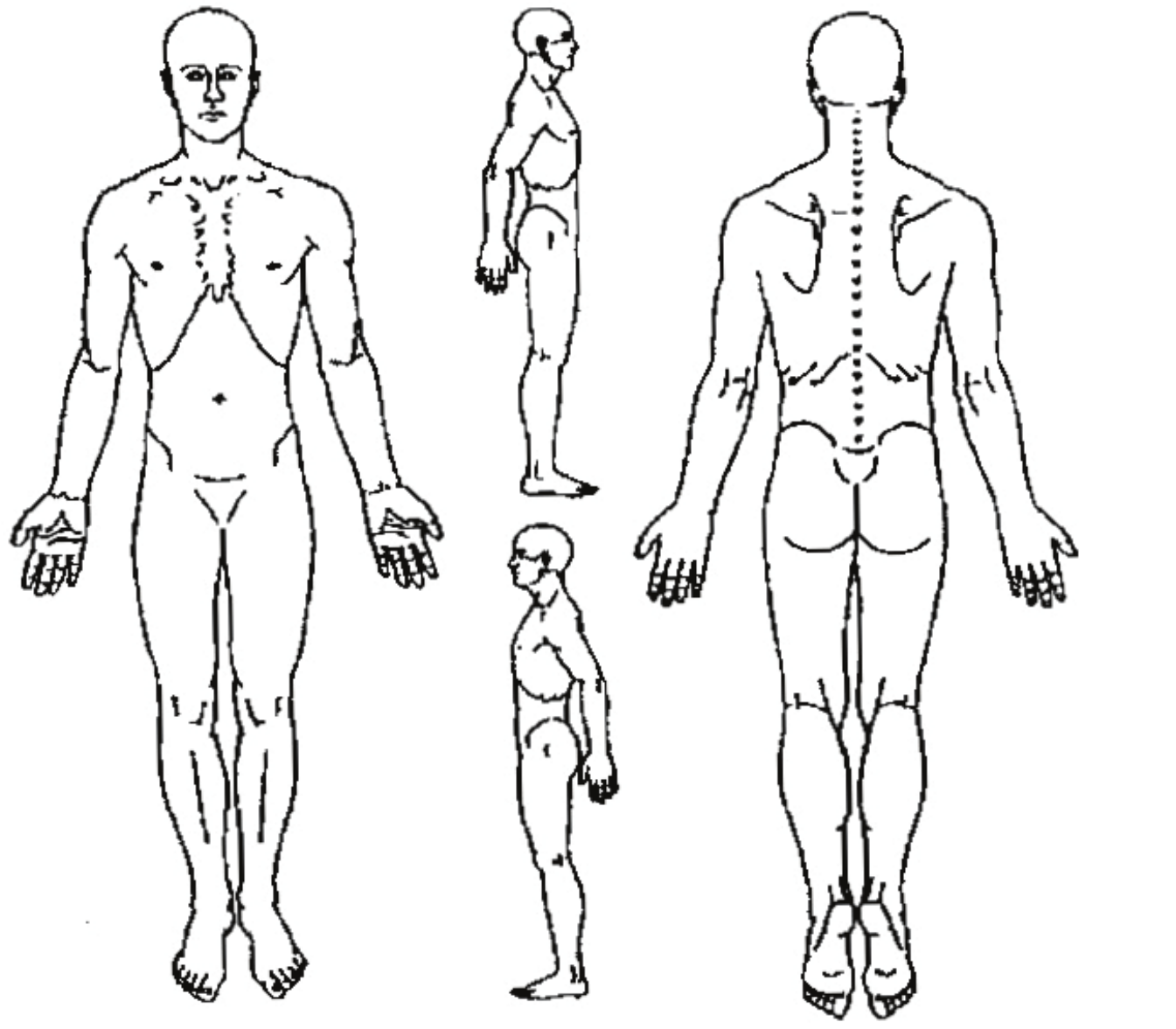
DRAW IN AREAS OF PAIN ON BODY DIAGRAMS USING APPROPRIATE SYMBOLS. If you are completing this form on the
computer, print form after completion and mark the diagram with a pen.
Patient#_______________ Provider_______
SEVERE PAIN *******
MODERATE PAIN 00000000
DULL ACHE ∩∩∩∩∩∩
RADIATING PAIN ↑↓↑↓↑↓↑↓
NUMBNESS/TINGLING XXXXXX
MEDICAL INFORMATION (MARK ALL THAT APPLY) **THIS INFORMATION IS CONFIDENTIAL AND REMAINS PART OF
YOUR CHART
DIFFICULTY SWALLOWING MOTION SICKNESS STROKE
ARTHRITIS FEVER/CHILLS/SWEATS OSTEOPOROSIS
HIGH BLOOD PRESSURE UNEXPLAINED WEIGHT LOSS ANEMIA
HEART TROUBLE BLOOD CLOTS BLEEDING PROBLEMS
PACEMAKER SHORTNESS OF BREATH HIV/HEPATITIS
EPILEPSY/SEIZURES HISTORY OF SMOKING HISTORY OF ALCOHOL ABUSE
HISTORY OF DRUG ABUSE DIABETES DEPRESSION/ANXIETY
MYOFASCIAL PAIN FIBROMYALGIA PREGNANCY
CANCER
PREVIOUS SURGERIES:_____________________________________________________________________________________________
OTHER:___________________________________________________________________________________________________________
MEDICATIONS:
__________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________
ALLERGIES:_______________________________________________________________________________________________________


