
Fillable Printable Post Sports-Related Head Injury Medical Clearance and Authorization Form - Massachusetts
Fillable Printable Post Sports-Related Head Injury Medical Clearance and Authorization Form - Massachusetts
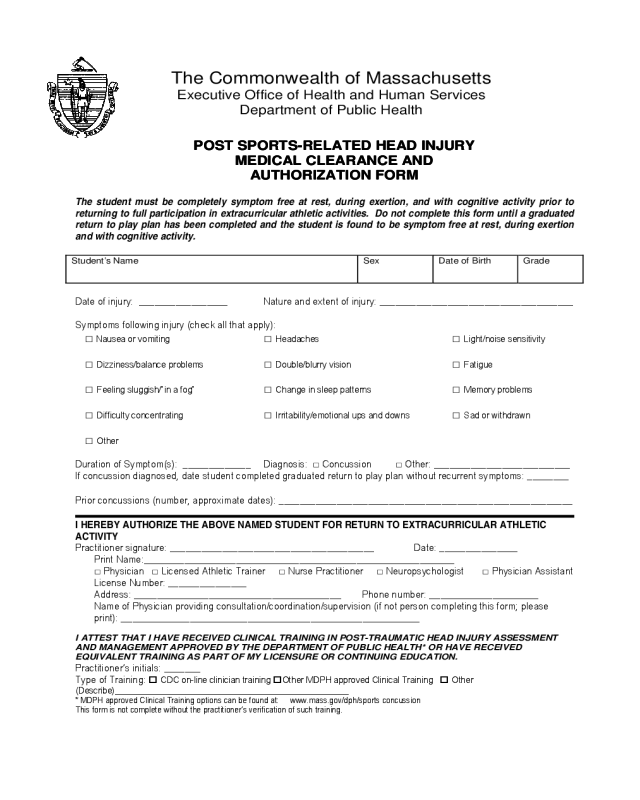
Post Sports-Related Head Injury Medical Clearance and Authorization Form - Massachusetts
The student must be completely symptom free at rest, during exertion, and with cognitive activity prior to
returning to full participation in extracurricular athletic activities. Do not complete this form until a graduated
return to play plan has been completed and the student is found to be symptom free at rest, during exertion
and with cognitive activity.
Student’s Name Sex Date of Birth Grade
Date of injury: _________________ Nature and extent of injury: _____________________________________
Symptoms following injury (check all that apply):
□ Nausea or vomiting □ Headaches □ Light/noise sensitivity
□ Dizziness/balance problems □ Double/blurry vision □ Fatigue
□ Feeling sluggish/”in a fog” □ Change in sleep patterns □ Memory problems
□ Difficulty concentrating □ Irritability/emotional ups and downs □ Sad or withdrawn
□ Other
Duration of Symptom(s): _____________ Diagnosis: □ Concussion □ Other: __________________________
If concussion diagnosed, date student completed graduated return to play plan without recurrent symptoms: ________
Prior concussions (number, approximate dates): ________________________________________________________
I HEREBY AU THORIZE THE ABOVE NAMED STUDENT FOR RETURN TO EXTRACURRICULAR ATHLETIC
ACTIVITY
Practitioner signature: _______________________________________ Date: _______________
Print Name:______________________________________________________
□ Physician □ Licensed Athletic Trainer □ Nurse Practitioner □ Neuropsychologist □ Physician Assistant
License Number: _______________
Address: ____________________________________ Phone number: ___________________
Name of Physician providing consultation/coordination/supervision (if not person completing this form; please
print): ____________________________________________________
I ATTEST THAT I HAVE RECEIVED CLINICAL TRAINING IN POST-TRAUMATIC HEAD INJURY ASSESSMENT
AND MANAGEMENT APPROVED BY THE DEPARTMENT OF PUBLIC HEALTH* OR HAVE RECEIVED
EQUIVALENT TRAINING AS PART OF MY LICENSURE OR CONTINUING EDUCATION.
Practitioner’s initials: _______
Type of Training:
CDC on-line clinician training Other MDPH approved Clinical Training Other
(Describe)_________________________________________________
* MDPH approved Clinical Training options can be found at: www.mass.gov/dph/sports concussion
This form is not complete without the practitioner’s verification of such training.
The Commonwealth of Massachusetts
Executive Office of Health and Human Services
Department of Public Health
POST SPORTS-RELATED HEAD INJURY
MEDICAL CLEARANCE AND
AUTHORIZATION FORM


