
Fillable Printable Request for Change of Address / Cancellation of Direct Deposit
Fillable Printable Request for Change of Address / Cancellation of Direct Deposit
Request for Change of Address / Cancellation of Direct Deposit
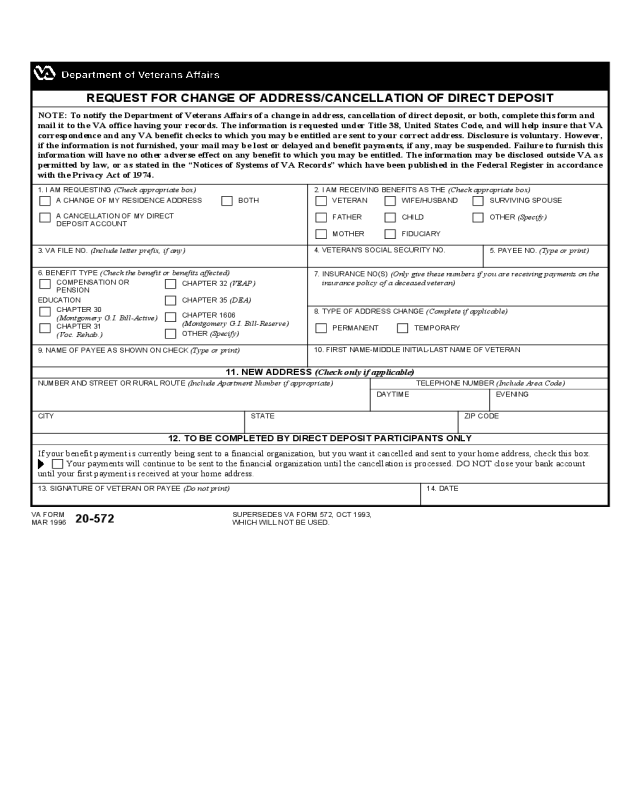
If your benefit payment is currently being sent to a financial organization, but you want it cancelled and sent to your home address, check this box.
Your payments will continue to be sent to the financial organization until the cancellation is processed. DO NOT close your bank account
until your first payment is received at your home address.
REQUEST FOR CHANGE OF ADDRESS/CANCELLATION OF DIRECT DEPOSIT
NOTE: To notify the Department of Veterans Affairs of a change in address, cancellation of direct deposit, or both, complete this form and
mail it to the VA office having your records. The information is requested under Title 38, United States Code, and will help insure that VA
correspondence and any VA benefit checks to which you may be entitled are sent to your correct address. Disclosure is voluntary. However,
if the information is not furnished, your mail may be lost or delayed and benefit payments, if any, may be suspended. Failure to furnish this
information will have no other adverse effect on any benefit to which you may be entitled. The information may be disclosed outside VA as
permitted by law, or as stated in the “Notices of Systems of VA Records” which have been published in the Federal Register in accordance
with the Privacy Act of 1974.
EDUCATION
SUPERSEDES VA FORM 572, OCT 1993,
WHICH WILL NOT BE USED.
3. VA FILE NO. (Include letter prefix, if any)
4. VETERAN'S SOCIAL SECURITY NO.
11. NEW ADDRESS (Check only if applicable)
1. I AM REQUESTING (Check appropriate box) 2. I AM RECEIVING BENEFITS AS THE (Check appropriate box)
A CHANGE OF MY RESIDENCE ADDRESS BOTH
FATHER
MOTHER
A CANCELLATION OF MY DIRECT
DEPOSIT ACCOUNT
5. PAYEE NO. (Type or print)
6. BENEFIT TYPE (Check the benefit or benefits affected)
7. INSURANCE NO(S) (Only give these numbers if you are receiving payments on the
insurance policy of a deceased veteran)
8. TYPE OF ADDRESS CHANGE (Complete if applicable)
9. NAME OF PAYEE AS SHOWN ON CHECK (Type or print)
10. FIRST NAME-MIDDLE INITIAL-LAST NAME OF VETERAN
CITY STATE ZIP CODE
14. DATE
PERMANENT TEMPORARY
COMPENSATION OR
PENSION
CHAPTER 30
(Montgomery G.I. Bill-Active)
CHAPTER 31
(Voc. Rehab.)
CHAPTER 32 (VEAP)
CHAPTER 35 (DEA)
CHAPTER 1606
(Montgomery G.I. Bill-Reserve)
CHILD
OTHER
(Specify)
SURVIVING SPOUSEWIFE/HUSBAND
FIDUCIARY
VETERAN
OTHER (Specify)
NUMBER AND STREET OR RURAL ROUTE (Include Apartment Number if appropriate) TELEPHONE NUMBER (Include Area Code)
DAYTIME EVENING
12. TO BE COMPLETED BY DIRECT DEPOSIT PARTICIPANTS ONLY
13. SIGNATURE OF VETERAN OR PAYEE (Do not print)
20-572
VA FORM
MAR 1996


