
Fillable Printable Sole Custody Worksheet - Colorado
Fillable Printable Sole Custody Worksheet - Colorado
Sole Custody Worksheet - Colorado
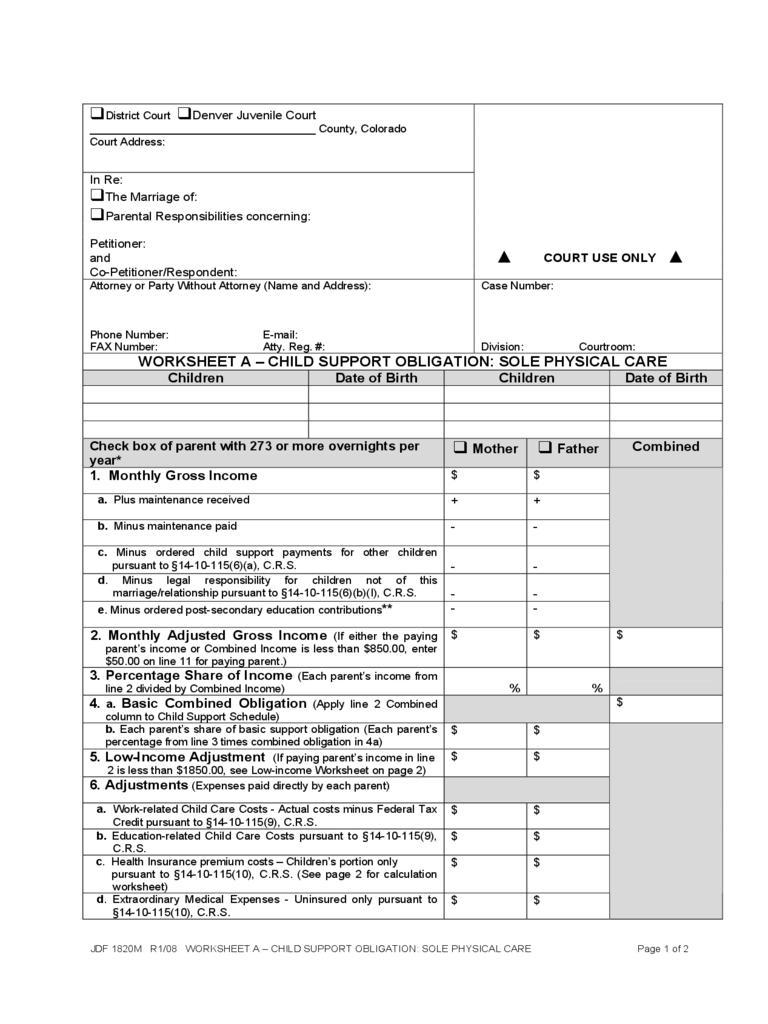
JDF 1820M R1/08 WORKSHEET A – CHILD SUPPORT OBLIGATION: SOLE PHYSICAL CARE Page 1 of 2
District Court Denver Juvenile Court
____________________________________ County, Colorado
Court Address:
In Re:
The Marriage of:
Parental Responsibilities concerning:
Petitioner:
and
Co-Petitioner/Respondent:
COURT USE ONLY
Attorney or Party Without Attorney (Name and Address): Case Number:
Phone Number: E-mail:
FAX Number: Atty. Reg. #: Division: Courtroom:
WORKSHEET A – CHILD SUPPORT OBLIGATION: SOLE PHYSICAL CARE
Children Date of Birth Children Date of Birth
Check box of parent with 273 or more overnights per
year*
Mother Father
Combined
1. Monthly Gross Income
$ $
a. Plus maintenance received
+ +
b. Minus maintenance paid
- -
c. Minus ordered child support payments for other children
pursuant to §14-10-115(6)(a), C.R.S.
-
-
d. Minus legal responsibility for children not of this
marriage/relationship pursuant to §14-10-115(6)(b)(I), C.R.S.
-
-
e. Minus ordered post-secondary education contributions**
- -
2. Monthly Adjusted Gross Income (If either the paying
parent’s income or Combined Income is less than $850.00, enter
$50.00 on line 11 for paying parent.)
$ $ $
3. Percentage Share of Income (Each parent’s income from
line 2 divided by Combined Income)
%
%
4. a. Basic Combined Obligation (Apply line 2 Combined
column to Child Support Schedule)
$
b. Each parent’s share of basic support obligation (Each parent’s
percentage from line 3 times combined obligation in 4a)
$ $
5. Low-Income Adjustment (If paying parent’s income in line
2 is less than $1850.00, see Low-income Worksheet on page 2)
$ $
6. Adjustments (Expenses paid directly by each parent)
a. Work-related Child Care Costs - Actual costs minus Federal Tax
Credit pursuant to §14-10-115(9), C.R.S.
$ $
b. Education-related Child Care Costs pursuant to §14-10-115(9),
C.R.S.
$ $
c. Health Insurance premium costs – Children’s portion only
pursuant to §14-10-115(10), C.R.S. (See page 2 for calculation
worksheet)
$ $
d. Extraordinary Medical Expenses - Uninsured only pursuant to
§14-10-115(10), C.R.S.
$ $
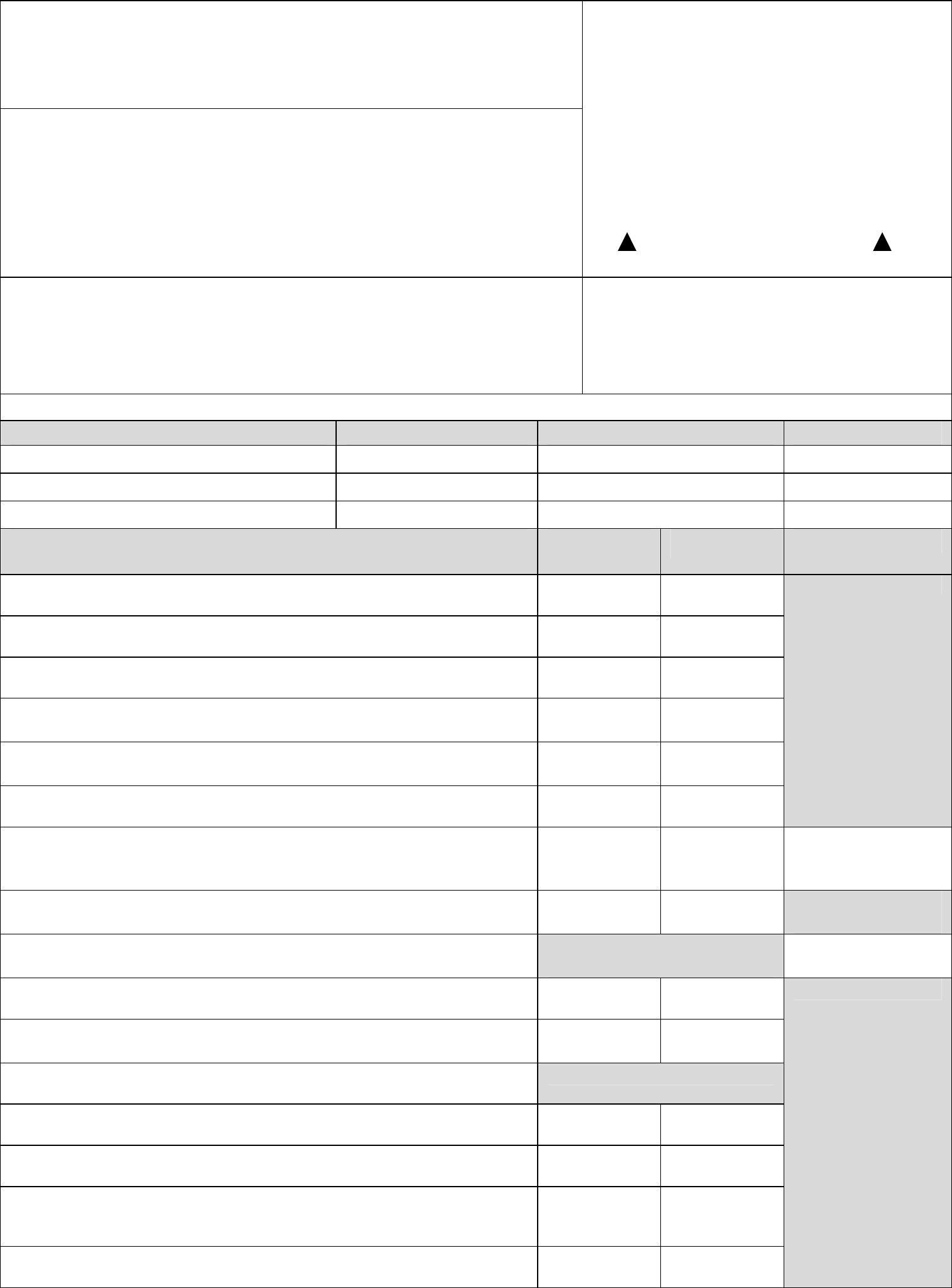
JDF 1820M R1/08 WORKSHEET A – CHILD SUPPORT OBLIGATION: SOLE PHYSICAL CARE Page 2 of 2
e. Extraordinary Expenses - Agreed to by parents or by order of
the Court pursuant to §14-10-115(11)(a), C.R.S.
$ $
f. Minus Extraordinary Adjustments pursuant to §14-10-115(11)(b),
C.R.S.
$ $
7. Total Adjustments (For each column, add 6a, 6b, 6c, 6d and
6e. Subtract line 6f then add two totals for Combined column
amount
)
$ $ $
8. Each Parent’s Fair Share of Adjustments (Line 7
Combined column times line 3 for each parent)
$ $
9. Each Parent’s Share of Total Child Support
Obligation
(Add lines 4b (or line 5 if less) and line 8 for each
parent)
$ $
10. Paying Parent’s Adjustment (Enter line 7 for parent
with less parenting time only)
$ $
11. Recommended Child Support Order (Subtract line 10
from line 9 for the paying parent only. Leave receiving parent
column blank)
$ $
Comments:
*The children reside with one parent for 273 or more overnights per year. If this is not the case, use Worksheet B.
**This adjustment applies only to modification of child support orders entered between 7/1/91 and 7/1/97 that provide
for post-secondary education expenses pursuant to § 14-10-115(15)(c), C.R.S.
Prepared by:
Signature: ________________________________Print Name: ___________________________
Date:
Low-Income Adjustment Worksheet
If the parents’ combined monthly adjusted gross income is more than $850.00 and the monthly adjusted gross income
of the parent with fewer overnights per year is less than $1850.00, use this calculation worksheet to determine the
adjustment allowed for that parent.
Low-income Adjustment Calculation
Adjusted monthly gross income of parent with fewer overnights (paying parent) from line 2
$ minus $900.00 = $ times 40% (.40) = $
Plus one of the following, according to number of children
1 child = $75.00 2 children = $150.00 3 children = $225.00
4 children = $275.00 5 children = $325.00 6 or more children = $350.00 + $
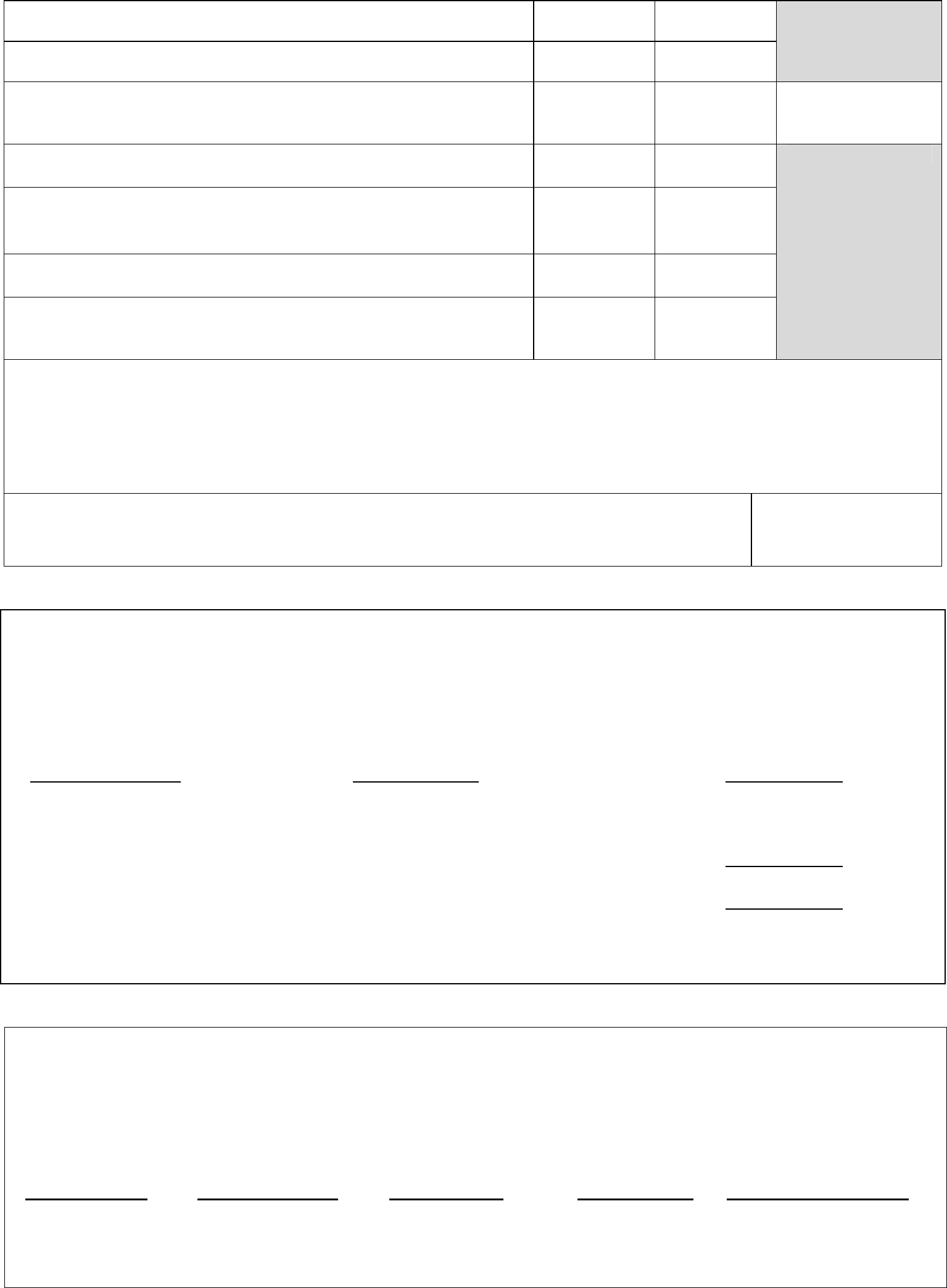
Low-income adjustment amount (#5 on worksheet) $
If this amount is less than the amount on line 4b (on page 1) for the parent with fewer overnights per year, this parent
qualifies for the Low-income Adjustment. Enter this amount on line 5 in that parent’s column on page 1. If this
number is a negative or zero, enter zero.
Heath Insurance Premium Calculation
If the actual amount of the health insurance premium that is attributable to the child(ren) who are the subject of
this order is not available or cannot be verified, the total cost of the premium should be divided by the number of
persons covered by the policy to determine a per person cost. This amount is then multiplied by the number of
children who are the subject of this order and are covered by the policy. This amount is then entered on line 6c on
page 1 of this form.
$ ÷ = $ x =
Total Number of Per Person Cost Number of Children’s Portion of
Premium Persons Covered Children Who Cost of Health
by the Policy Are the Subject Insurance Premium
of this Order (Enter on line 6c)


