
Fillable Printable Standard Employee Status Change Form
Fillable Printable Standard Employee Status Change Form
Standard Employee Status Change Form
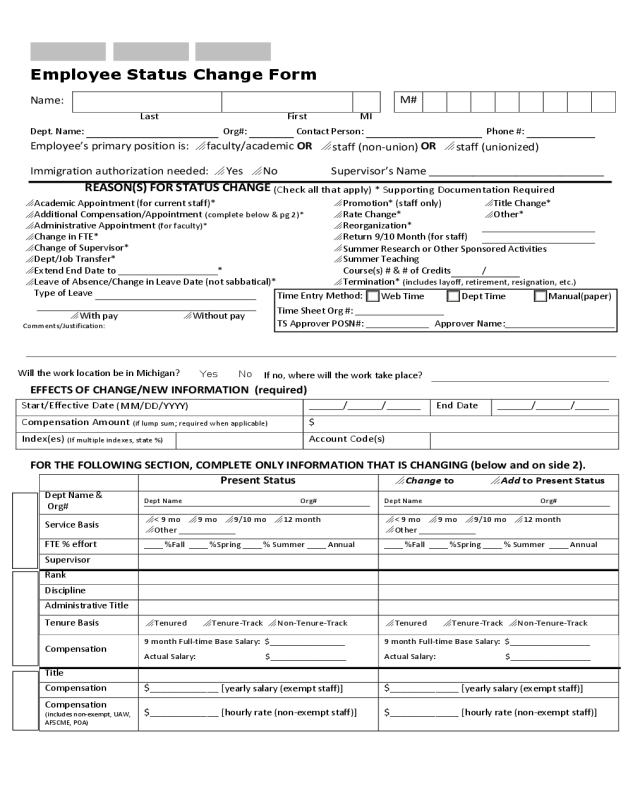
Employee Status Change Form
Name:
M#
Last First MI
Dept. Name: Org#: Contact Person: Phone #:
Employee’s primary position is:
faculty/academic OR
staff (non-union)
OR
staff (unionized)
Immigration authorization needed:
Yes
No Supervisor’s Name ____________________________
REASON(S) FOR STATUS CHANGE
(Check all that apply) * Supporting Documentation Required
Academic Appointment (for current staff)*
Promotion* (staff only)
Title Change*
Additional Compensation/Appointment
(complete below & pg 2)*
Rate Change*
Other*
Administrative Appointment
(for faculty)*
Reorganization*
Change in FTE*
Return 9/10 Month (for staff)
Change of Supervisor*
Summer Research or Other Sponsored Activities
Dept/Job Transfer*
Summer Teaching
Extend End Date to ___________________* Course(s) # & # of Credits /
Leave of Absence/Change in Leave Date (not sabbatical)*
Termination*
(includes layoff, retirement, resignation, etc.)
Type of Leave
With pay
Without pay
Comments/Justification:
EFFECTS OF CHANGE/NEW INFORMATION (required)
Start/Effective Date
(MM/DD/YYYY)
______/______/______ End Date ______/______/______
Compensation Amount
(if lump sum; required when applicable)
$
Index(es)
(If multiple indexes, state %)
Account Code(s)
FOR THE FOLLOWING SECTION, COMPLETE ONLY INFORMATION THAT IS CHANGING (below and on side 2).
Present Status
Change to
Add to Present Status
Dept Name &
Org#
Dept Name Org# Dept Name Org#
Service Basis
< 9 mo
9 mo
9/10 mo
12 month
Other ____________
< 9 mo
9 mo
9/10 mo
12 month
Other ____________
FTE % effort
____ %Fall ____ %Spring ____ % Summer ____ Annual ____ %Fall ____ %Spring ____ % Summer ____ Annual
Supervisor
Rank
Discipline
Administrative Title
Tenure Basis
Tenured
Tenure-Track
Non-Tenure-Track
Tenured
Tenure-Track
Non-Tenure-Track
Compensation
9 month Full-time Base Salary: $________________
Actual Salary: $________________
9 month Full-time Base Salary: $_________________
Actual Salary: $_________________
Title
Compensation $____________ [
yearly salary (exempt staff)]
$____________ [
yearly salary (exempt staff)]
Compensation
(includes non-exempt, UAW,
AFSCME, POA)
$____________ [
hourly rate (non-exempt staff)]
$____________ [
hourly rate (non-exempt staff)]
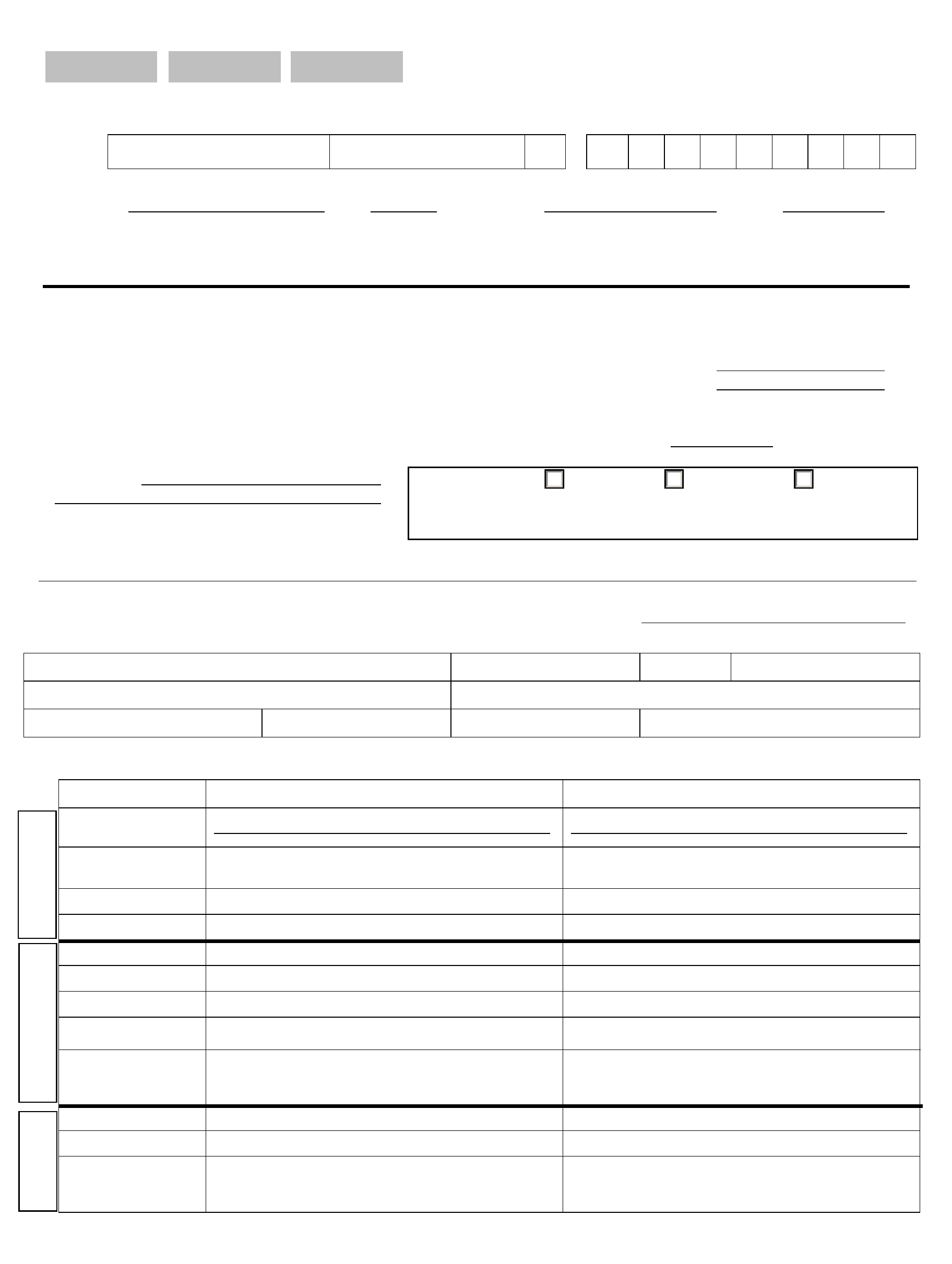
Time Entry Method:
Web Time Dept Time Manual(paper)
Time Sheet Org #: _________________
TS Approver POSN#: ____________
Approver Name:_____________________
Will the work location be in Michigan?
Yes No
If no, where will the work take place?
ADDITIONAL COMPENSATION (Signature required through Vice President) – HR will complete account codes
Additional Compensation (documentation required) – Compensation for additional work performed
Eligible employees must be full-time faculty or full-time exempt staff.
Additional compensation requests must be processed before work is performed. After-the-fact requests from sponsored accounts will not be
recognized.
Complete information below only if employee is receiving additional compensation.
Is employee currently being paid
from a sponsored account?
Yes
No
Is it anticipated that the employee will be paid from a
sponsored account during the time period requested?
Yes
No
Notes (if additional
course is being taught,
include course #)
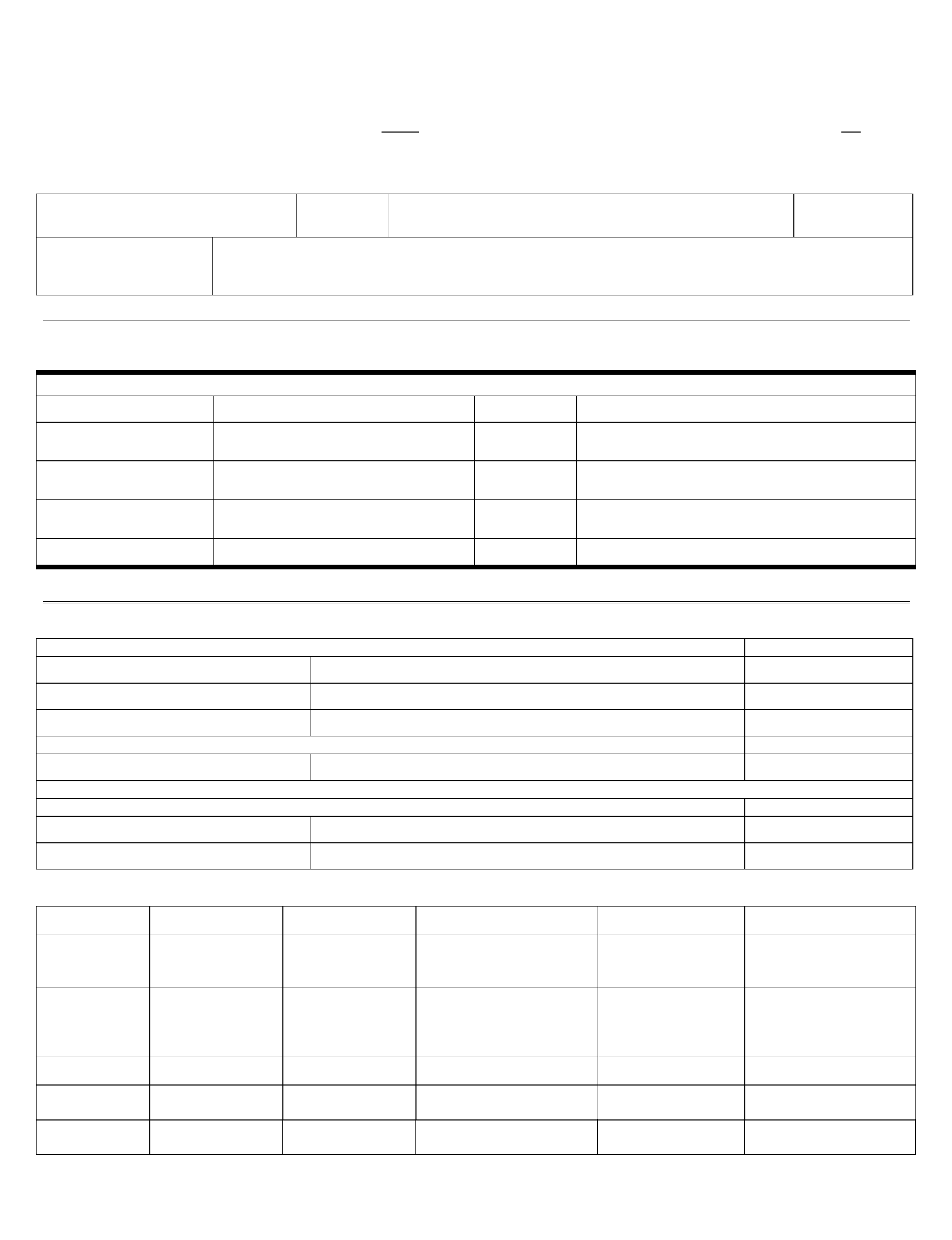
APPROVALS/REVIEWS
For all changes, two levels of approvals are needed (not including Financial Manager); HR will obtain executive signatures when necessary.
Department/College/School
Print Name Signature Date Supervisory Approvals
Financial Manager / Dept Chair / Supervisor
(or Designee with approval)
Next highest in supervisory chain of command
(if not Dean/Director)
Dept Chair/Supervisor
(only if dual appointment or
other department is responsible for payment)
Dean/Director
(mandatory – if applicable)
Forward completed form to Human Resources
For Internal Use Only
Compliance Review Date
Human Resources
*
Office of Institutional Equity
Sponsored Programs Accounting (index check if sponsored account)
Compliance with Sponsor Guidelines (only if applicable) Date
Sponsored Programs Office
Approval from sponsor received.
Final Approvals – Obtained by HR Date
Executive Team Member
President
For HR Use Only
Position # Pay Grade JERC Code
Position Class Pay Rate Additional
Compensation
Supplementary
Non-recurring
Intra-Univ Consulting
Employee Class Step Leave of Absence
Paid
Unpaid
With benefits
Without benefits
Leave Category Home Dept Org to: Change Supervisor to:
Benefit Category Time Sheet Org to: Date Requested
Revised Org Chart:
SOC Code:
CUPA Code:
Job Group:
__ __ - __ __ __ __
__ __ __
_____________Copied * Leave of Absence Approval – Benefits Office ____________________________________ |
Form Updated 04/28/15


