
Fillable Printable Straight Bill of Lading
Fillable Printable Straight Bill of Lading
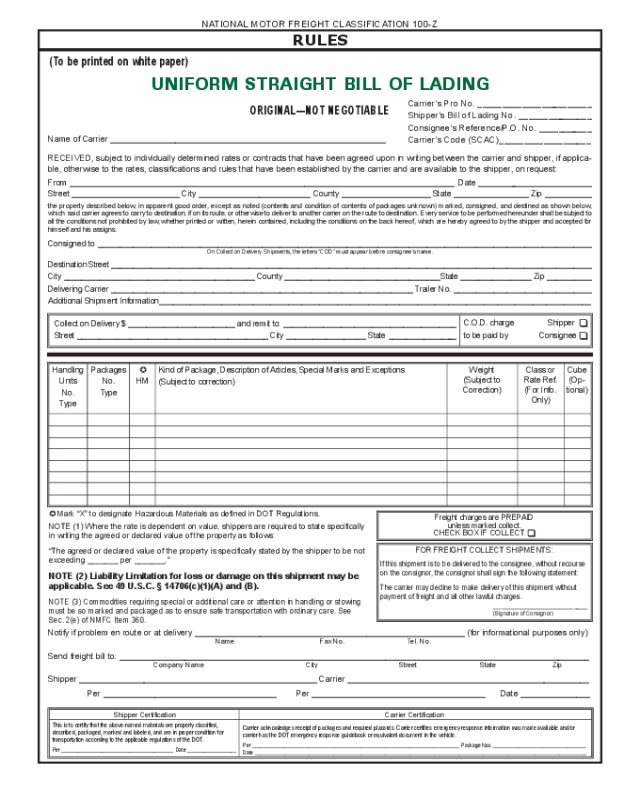
Straight Bill of Lading

(To be printed on white paper)
UNIFORM STRAIGHT BILL OF LADING
ORIGINAL—NOT NEGOTIABLE
RULES
NATIONAL MOTOR FREIGHT CLASSIFICATION 100-Z
Carrier’s Pro No. ________________________
Shipper’s Bill of Lading No. ________________
Consignee’s Reference/P.O. No. ____________
Carrier’s Code (SCAC)___________________
Name of Carrier ___________________________________________________________
RECEIVED, subject to individually determined rates or contracts that have been agreed upon in writing between the carrier and shipper, if applica-
ble, otherwise to the rates, classifications and rules that have been established by the carrier and are available to the shipper, on request:
From __________________________________________________________________________________ Date _________________________
Street _______________________ City ________________________ County ___________________ State ________________ Zip __________
the property described below, in apparent good order, except as noted (contents and condition of contents of packages unknown) marked, consigned, and destined as shown below,
which said carrier agrees to carry to destination, if on its route, or otherwise to deliver to another carrier on the route to destination. Every service to be performed hereunder shall be subject to
all the conditions not prohibited by law, whether printed or written, herein contained, including the conditions on the back hereof, which are hereby agreed to by the shipper and accepted for
himself and his assigns.
Consigned to _______________________________________________________________________________________________________________
On Collect on Delivery Shipments, the letters “COD” must appear before consignee’s name.
Destination Street ____________________________________________________________________________________________________________
City ___________________________________________ County ___________________________________State ________________ Zip __________
Delivering Carrier ____________________________________________________________________ Trailer No. _______________________________
Additional Shipment Information_________________________________________________________________________________________________
Collect on Delivery $ ________________________ and remit to: _______________________________________
Street ___________________________________________ City __________________ State ________________
C.O.D. charge Shipper T
to be paid by Consignee T
Handling
Units
No.
Type
Packages
No.
Type
-
HM
Kind of Package, Description of Articles, Special Marks and Exceptions
(Subject to correction)
Weight
(Subject to
Correction)
Class or
Rate Ref.
(For Info.
Only)
Cube
(Op-
tional)
Freight charges are PREPAID
unless marked collect.
CHECK BOX IF COLLECT T
FOR FREIGHT COLLECT SHIPMENTS:
If this shipment is to be delivered to the consignee, without recourse
on the consignor, the consignor shall sign the following statement:
The carrier may decline to make delivery of this shipment without
payment of freight and all other lawful charges.
_________________________
(Signature of Consignor)
- Mark “X” to designate Hazardous Materials as defined in DOT Regulations.
NOTE (1) Where the rate is dependent on value, shippers are required to state specifically
in writing the agreed or declared value of the property as follows:
“The agreed or declared value of the property is specifically stated by the shipper to be not
exceeding _______ per _______.”
NOTE (2) Liability Limitation for loss or damage on this shipment may be
applicable. See 49 U.S.C. § 14706(c)(1)(A) and (B).
NOTE (3) Commodities requiring special or additional care or attention in handling or stowing
must be so marked and packaged as to ensure safe transportation with ordinary care. See
Sec. 2(e) of NMFC Item 360.
Notify if problem en route or at delivery __________________________________________________________ (for informational purposes only)
Name Fax No. Tel. No.
Send freight bill to: _____________________________________________________________________________________________________
Company Name City Street State Zip
Shipper ___________________________________________________ Carrier ____________________________________________________
Per _____________________________________ Per _____________________________________ Date _______________
Shipper Certification
This is to certify that the above-named materials are properly classified,
described, packaged, marked and labeled, and are in proper condition for
transportation according to the applicable regulations of the DOT.
Per _________________________________________ Date __________________
Carrier Certification
Carrier acknowledges receipt of packages and required placards. Carrier certifies emergency response information was made available and/or
carrier has the DOT emergency response guidebook or equivalent document in the vehicle.
Per ____________________________________________________________________________ Package Nos. __________________________________
Date __________________________________________________________________________________________________________________________


