
Fillable Printable Student Emergency Release Authorization Form
Fillable Printable Student Emergency Release Authorization Form
Student Emergency Release Authorization Form
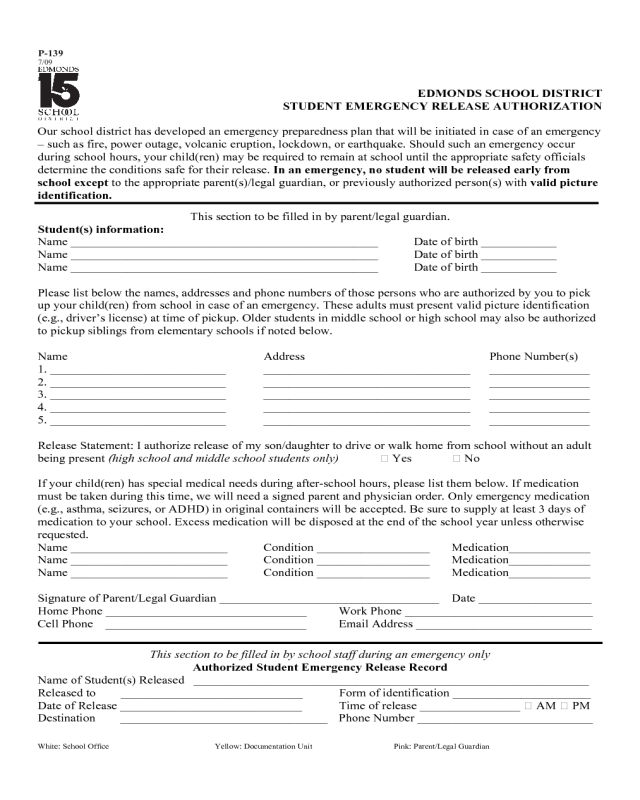
EDMONDS SCHOOL DISTRICT
STUDENT EMERGENCY RELEASE AUTHORIZATION
White: School Office Yellow: Documentation Unit Pink: Parent/Legal Guardian
Our school district has developed an emergency preparedness plan that will be initiated in case of an emergency
– such as fire, power outage, volcanic eruption, lockdown, or earthquake. Should such an emergency occur
during school hours, your child(ren) may be required to remain at school until the appropriate safety officials
determine the conditions safe for their release. In an emergency, no student will be released early from
school except to the appropriate parent(s)/legal guardian, or previously authorized person(s) with valid picture
identification.
This section to be filled in by parent/legal guardian.
Student(s) information:
Name _________________________________________________ Date of birth ____________
Name _________________________________________________ Date of birth ____________
Name _________________________________________________ Date of birth ____________
Please list below the names, addresses and phone numbers of those persons who are authorized by you to pick
up your child(ren) from school in case of an emergency. These adults must present valid picture identification
(e.g., driver’s license) at time of pickup. Older students in middle school or high school may also be authorized
to pickup siblings from elementary schools if noted below.
Name Address Phone Number(s)
1. ____________________________ _________________________________ ________________
2. ____________________________ _________________________________ ________________
3. ____________________________ _________________________________ ________________
4. ____________________________ _________________________________ ________________
5. ____________________________ _________________________________ ________________
Release Statement: I authorize release of my son/daughter to drive or walk home from school without an adult
being present (high school and middle school students only) ͔ Yes ͔ No
If your child(ren) has special medical needs during after-school hours, please list them below. If medication
must be taken during this time, we will need a signed parent and physician order. Only emergency medication
(e.g., asthma, seizures, or ADHD) in original containers will be accepted. Be sure to supply at least 3 days of
medication to your school. Excess medication will be disposed at the end of the school year unless otherwise
requested.
Name _________________________ Condition __________________ Medication_____________
Name _________________________ Condition __________________ Medication_____________
Name _________________________ Condition __________________ Medication_____________
Signature of Parent/Legal Guardian ___________________________________ Date __________________
Home Phone ________________________________ Work Phone ______________________________
Cell Phone ________________________________ Email Address ____________________________
This section to be filled in by school staff during an emergency only
Authorized Student Emergency Release Record
Name of Student(s) Released _______________________________________________________________
Released to _____________________________ Form of identification ______________________
Date of Release _____________________________ Time of release ________________ ͔ AM ͔ PM
Destination _________________________________ Phone Number ____________________________
P-139
7/09


