
Fillable Printable Student Medical Form - Florida
Fillable Printable Student Medical Form - Florida
Student Medical Form - Florida
German Measles (Rubella)
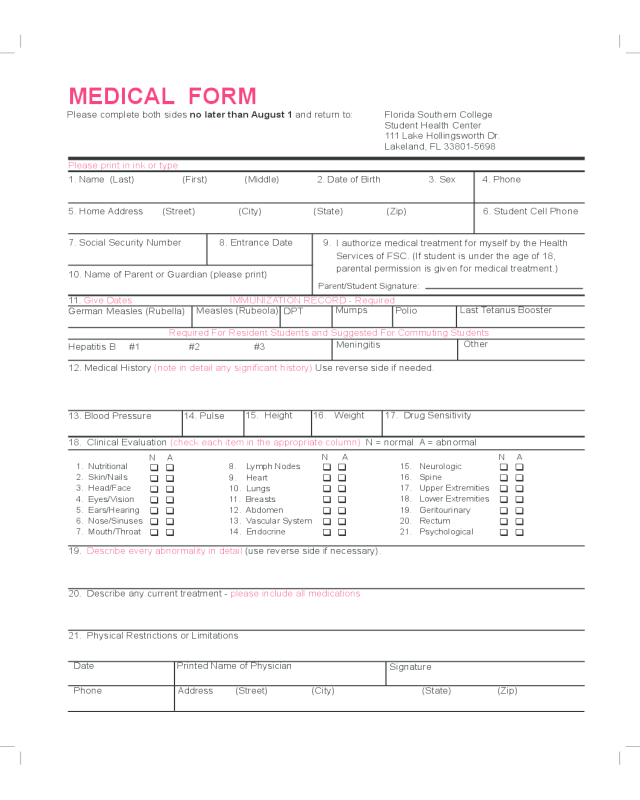
MEDICAL FORM
Please complete both sides no later than August 1 and return to: Florida Southern College
Student Health Center
111 Lake Hollingsworth Dr.
Lakeland, FL 33801-5698
1. Name (Last) (First) (Middle) 2. Date of Birth 3. Sex 4. Phone
5. Home Address (Street) (City) (State) (Zip) 6. Student Cell Phone
7. Social Security Number 8. Entrance Date 9.
10. Name of Parent or Guardian (please print)
I authorize medical treatment for myself by the Health
Services of FSC. (If student is under the age of 18,
parental permission is given for medical treatment.)
Please print in ink or type
12. Medical History (note in detail any signicant history) Use reverse side if needed.
Hepatitis B #1 #2 #3
Required For Resident Students and Suggested For Commuting Students
13. Blood Pressure
11. Give Dates IMMUNIZATION RECORD - Required
18. Clinical Evaluation (check each item in the appropriate column) N = normal A = abnormal
1. Nutritional
2. Skin/Nails
3. Head/Face
4. Eyes/Vision
5. Ears/Hearing
6. Nose/Sinuses
7. Mouth/Throat
8. Lymph Nodes
9. Heart
10. Lungs
11. Breasts
12. Abdomen
13. Vascular System
14. Endocrine
15. Neurologic
16. Spine
17. Upper Extremities
18. Lower Extremities
19. Geritourinary
20. Rectum
21. Psychological
N A
q q
q q
q q
q q
q q
q q
q q
N A
q q
q q
q q
q q
q q
q q
q q
19. Describe every abnormality in detail (use reverse side if necessary).
20. Describe any current treatment - please include all medications
21. Physical Restrictions or Limitations
Date
Phone Address (Street) (City) (State) (Zip)
Printed Name of Physician
Signature
17. Drug Sensitivity16. Weight 15. Height
14. Pulse
Other
Meningitis
Last Tetanus Booster
Polio
Mumps
DPT
Measles (Rubeola)
N A
q q
q q
q q
q q
q q
q q
q q
Parent/Student Signature:

I have read the information on meningitis and hepatitis B that the college provided.
I have received the vaccine on the following dates:
Meningitis vaccine:
(REQUIRED FOR ALL RESIDENTIAL STUDENTS)
Hepatitis B vaccine #1: #2 #3
I have elected to waive obtaining the following:
Hepatitis B vaccines
Meningitis vaccine
(THIS OPTION IS AVAILABLE ONLY TO COMMUTING STUDENTS)
Student signature Date
Parent signature if student Date
is under 18 years of age
q
q
q
q
Additional Space for Medical Form Data
MENINGITIS AND HEPATITIS FORM
Name SS# Date / /
Birth Date / / Sex M F Height Wt. Marital Status S M D W
Local Address Phone ( )
Permanent Address Phone ( )
To be completed by student PAST MEDICAL HISTORY Please print in ink or type.
Mark “X” if
you have had
Alcohol/drug dependence Heart problems
Allergy/hay fever Hemorrhoids
Anemia/blood disease Hepatitis
Anxiety High Blood Pressure
Arthritis/joint pain High cholesterol
Asthma Hypoglycemia
Back problem Insomnia
Bladder/kidney Liver disease/jaundice
Blood in stool Malaria
Cancer/cyst/tumor Mononucleosis
Clot in veins Pregnancy
Constipation Psychological problem
Depression Respiratory problem
Diabetes (sugar) Rheumatic fever
Diarrhea Sexually transmitted disease
Dizziness/fainting Shortness of breath
Ear & nose problem Skin problem
Epilespy/seizures Strep throat
Eye problem Swollen glands
Gallbladder/intestinal Swollen joints
Head injury Thyroid disease
Surgeries/hospitalization/injuries, list below: Tuberculosis
Ulcer
Varicose veins
Weight problem
Other:
Do you smoke? Yes No
How much per day?
Do you drink alcohol or use marijuana? Yes No Do you have any allergies to medication? Yes No
How much per day? If yes, please list:
Current medications:
Do you have any other allergies? Yes No
If yes , please list:
Mark “X” if
you have had
Date
Date
MEDICAL HISTORY FORM
Please complete no later than August 1 and return to: Florida Southern College
Student Health Center
111 Lake Hollingsworth Dr.
Lakeland, FL 33801-5698


