
Fillable Printable Upgrade & Optional/ Uncovered Treatment Form - California
Fillable Printable Upgrade & Optional/ Uncovered Treatment Form - California
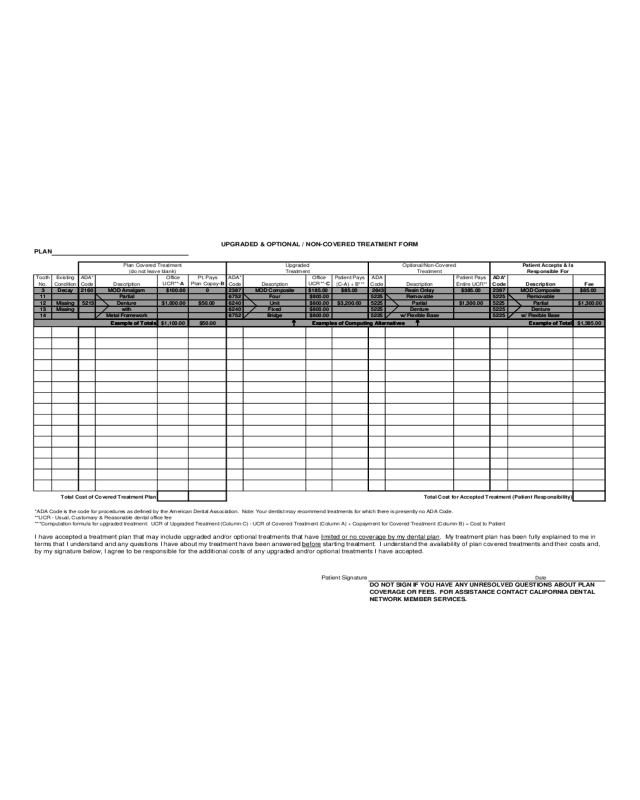
Upgrade & Optional/ Uncovered Treatment Form - California
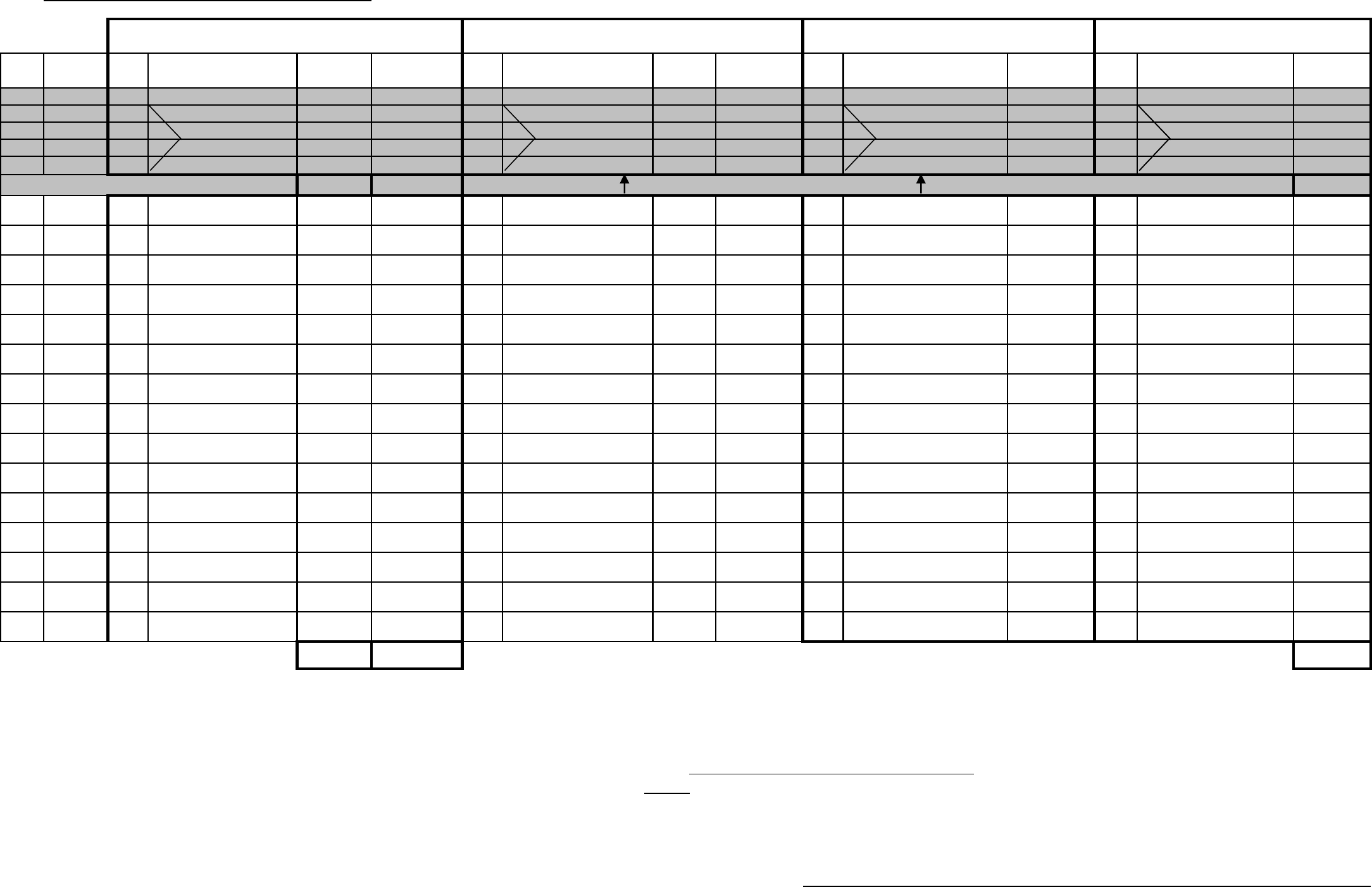
PLAN
Tooth Existi ng ADA* Off ice Pt. Pays ADA* Off ice Patient Pays ADA Patient Pays ADA*
No. Condition Code Description
UCR**-
A
Plan Copay- B
Code Description
UCR**-C
(C- A) + B*** Code Description Entir e UCR** Code Description Fee
3 Decay 2160 MOD Amalgam $100.00 0 2387 MOD Composite $185.00 $85.00 2643 Resin Onlay $385.00 2387 MOD Composite $85.00
11 Partial 6752 Four $800.00 5225 Removable 5225 Removable
12 Missing 5213 Denture $1,000.00 $50.00 6240 Unit $800.00 $3,200.00 5225 Partial $1,300.00 5225 Partial $1,300.00
13 Missing with 6240 Fixed $800.00 5225 Denture 5225 Denture
14 Metal Framework 6752 Bridge $800.00 5225 w/ Flexible Base 5225 w/ Flexible Base
$1,100.00 $50.00 $1,385.00
*ADA Code is t he code for procedures as defined by the Ameri can Dental Association. Note: Your dent ist may recommend treatments for which there is presently no ADA Code.
**UCR - Usual, Customary & Reasonable dental office fee
***Computation formula for upgraded treatment: UCR of Upgraded Treatment (Column C) - UCR of Covered Treat ment (Column A) + Copay ment for Covered T reatment (C olumn B) = Cost t o Patient
I have accepted a treatment plan that may include upgraded and/or optional treatments that have limited or no coverage by my de ntal plan . My treatment plan has been fully explained to me in
terms that I understand and any questions I have about my treatment have been answered before
starting treatment. I understand the availability of plan covered treatments and their costs and,
by my signature below, I agree to be responsible for the additional costs of any upgraded and/or optional treatments I have accepted.
Date
DO NOT SIGN IF YOU HAVE ANY UNRESOLVED QUESTIONS ABOUT PLAN
COVERAGE OR FEES. FOR ASSISTANCE CONTACT CALIFORNIA DENTAL
NETWORK MEMBER SERVICES.
UPGRAD ED & OPTIONAL / NON-COVERED TREATMENT FORM
Plan Covered Treatment
(do not leave bl ank)
Upgraded
Treatment
Pati ent Accepts & Is
Responsibl e For
Optional/Non-Covered
Treatment
Total Cost of Covered Treat ment Plan Total Cost for Accept ed Treatm ent (Patient Responsibility)
Patient Signature
Example of Totals Examples of Comput ing Alt ernatives Example of Total


