
Fillable Printable VA Form 10-7959f-2
Fillable Printable VA Form 10-7959f-2
VA Form 10-7959f-2
OMB Approval Number 2900-0648
Estimated Burden Avg: 11 minutes
Expiration Date: 03/31/2019
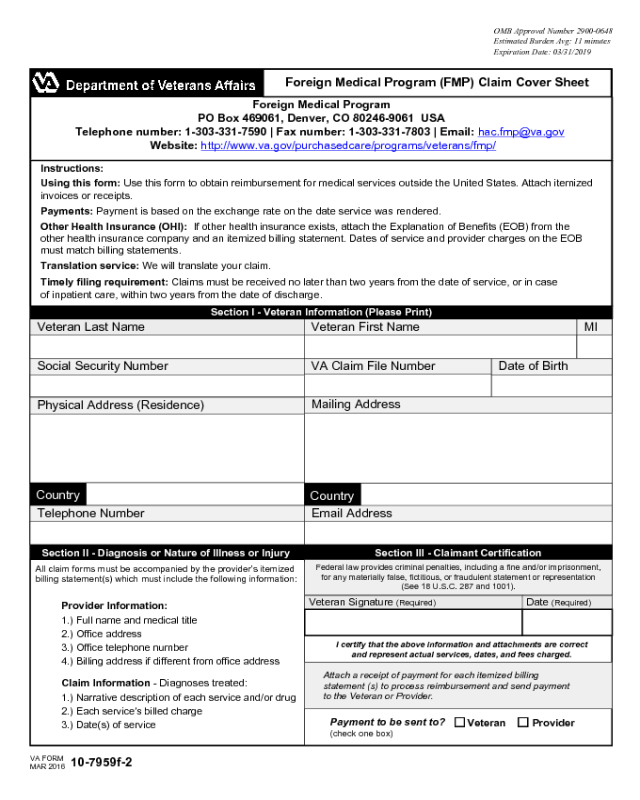
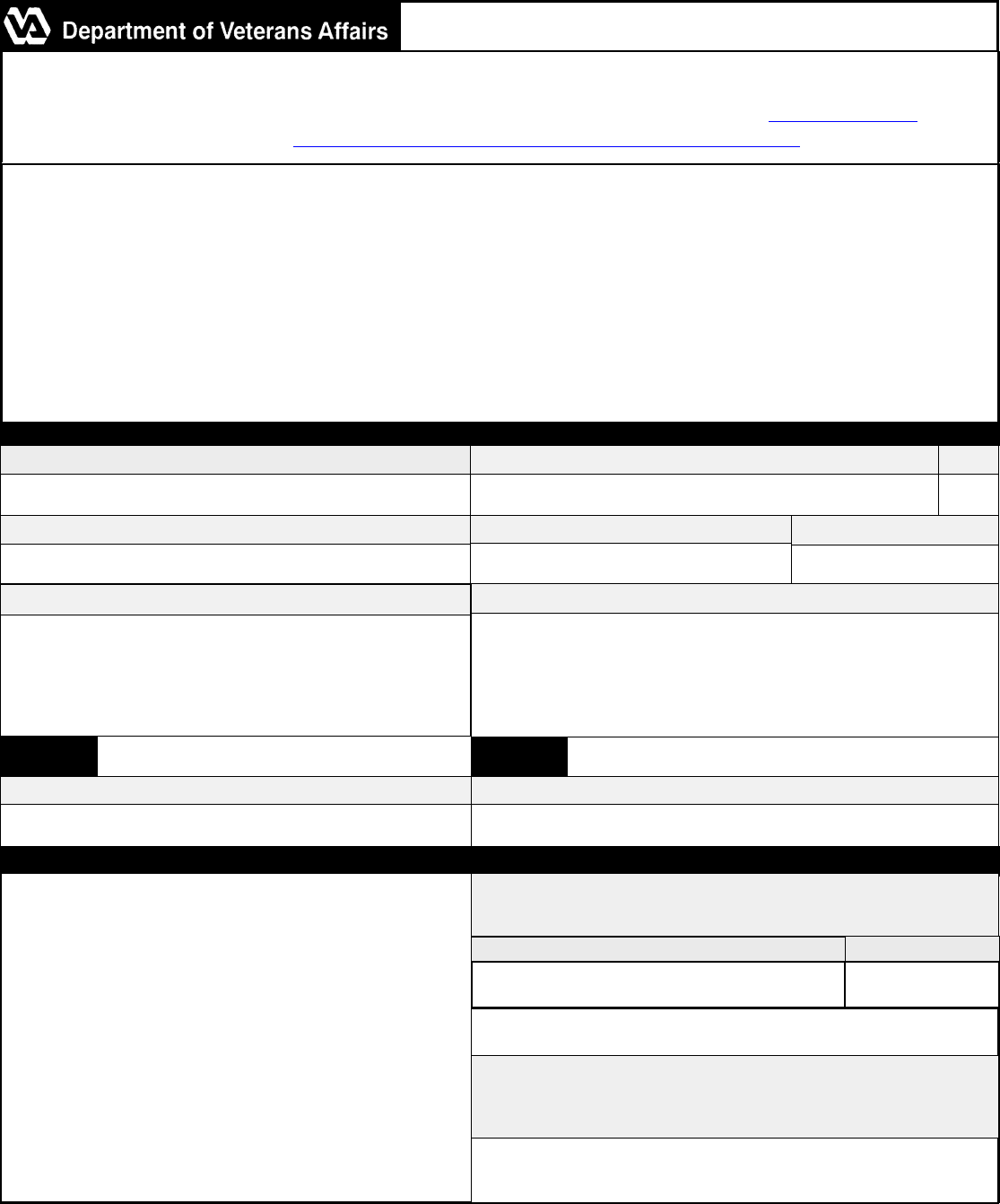
Foreign Medical Program
PO Box 469061, Denver, CO 80246-9061 USA
Telephone number: 1-303-331-7590 | Fax number: 1-303-331-7803 | Email: [email protected]
Website: http://www.va.gov/purchasedcare/programs/veterans/fmp/
Instructions:
Using this form: Use this form to obtain reimbursement for medical services outside the United States. Attach itemized
invoices or receipts.
Payments: Payment is based on the exchange rate on the date service was rendered.
Other Health Insurance (OHI): If other health insurance exists, attach the Explanation of Benefits (EOB) from the
other health insurance company and an itemized billing statement. Dates of service and provider charges on the EOB
must match billing statements.
Translation service: We will translate your claim.
Timely filing requirement: Claims must be received no later than two years from the date of service, or in case
of inpatient care, within two years from the date of discharge.
Section I - Veteran Information (Please Print)
Section II - Diagnosis or Nature of Illness or Injury
All claim forms must be accompanied by the provider’s itemized
billing statement(s) which must include the following information:
Provider Information:
1.) Full name and medical title
2.) Office address
3.) Office telephone number
4.) Billing address if different from office address
Claim Information - Diagnoses treated:
1.) Narrative description of each service and/or drug
2.) Each service’s billed charge
3.) Date(s) of service
Section III - Claimant Certification
Federal law provides criminal penalties, including a fine and/or imprisonment,
for any materially false, fictitious, or fraudulent statement or representation
(See 18 U.S.C. 287 and 1001).
Veteran Signature (Required) Date (Required)
I certify that the above information and attachments are correct
and represent actual services, dates, and fees charged.
Payment to be sent to?
(check one box)
Veteran Provider
VA FORM
MAR 2016
10-7959f-2
Veteran Last Name Veteran First Name MI
Social Security Number
VA Claim File Number
Physical Address (Residence)
Mailing Address
Country
Country
Telephone Number
Date of Birth
Email Address
Foreign Medical Program (FMP) Claim Cover Sheet
Attach a receipt of payment for each itemized billing
statement (s) to process reimbursement and send payment
to the Veteran or Provider.
Privacy Act and Paperwork Reduction Act Information: The information requested on this form is
solicited under the Authority: Title 38, U.S.C. 1724. The Systems of Records that apply are 23VA10NB3,
Non-VA Care (Fee) Records-VA (FR 80 No.146 July 30, 2015) and 54VA10NB3, (FR 80 No. 41, Mar 3,
2015) "Veterans and Beneficiaries Purchased Care Community Health Care Claims, Correspondence,
Eligibility, Inquiry and Payment Files --VA''. Purpose: Records may be used to establish, determine, and
monitor eligibility to receive VA benefits and for authorizing and paying Non-VA healthcare services
furnished to veterans and beneficiaries and to process claims for medical care and services, and to process
stipends. Principle: Veterans, Beneficiaries, Pensioned members of the allied forces and Healthcare
providers treating individuals who receive care under 38 U.S.C. Chapters 1 and 17. Routine Use: Routine
use disclosures are in accordance with the Privacy Act of 1974 (as amended) and the applicable system of
records notice. Disclosure: Your disclosure of the information requested on this form is voluntary. However,
if the information including Social Security number (SSN) (the SSN will be used to locate records) is not
furnished completely and accurately, Department of Veterans Affairs will be unable to comply with the
request. Not supplying the SSN may delay processing your claims. VA may disclose the information as a
routine use disclosure outlined in applicable Privacy Act Systems of Records Notice.
The Paperwork Reduction Act of 1995 requires us to notify you that this information collection is in
accordance with the clearance requirements of section 3507 of the Paperwork Reduction Act of 1995. We
may not conduct or sponsor and you are not required to respond to, a collection of information unless it
displays a valid OMB number. We anticipate that the time expended by all individuals who must complete
this form will average 11 minutes. This includes the time it will take to read instructions, gather the necessary
facts and fill out the form.
VA FORM
MAR 2016
10-7959f-2
Foreign Medical Program (FMP) Claim Cover Sheet


