
Fillable Printable WIC Medical Referral Form for Women - New York
Fillable Printable WIC Medical Referral Form for Women - New York
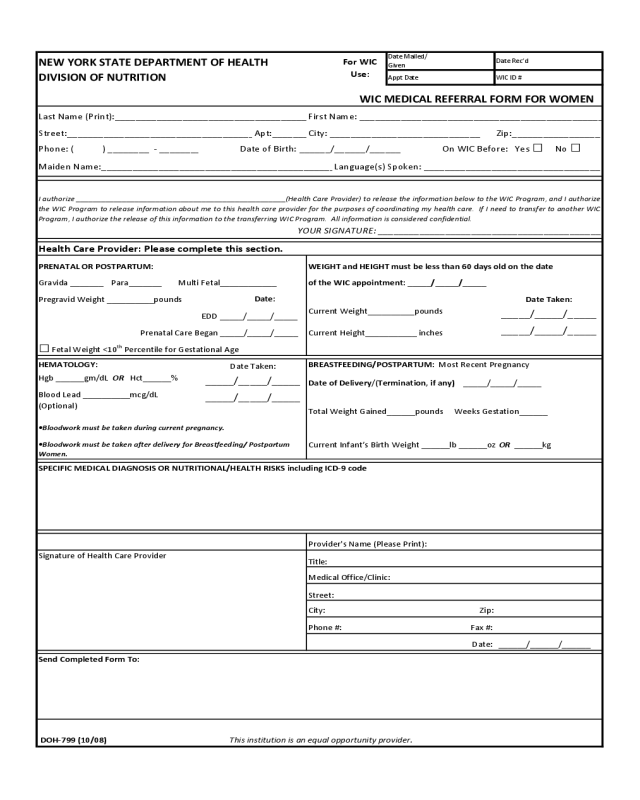
WIC Medical Referral Form for Women - New York
NEWYORKSTATEDEPARTMENTOFHEALTH
DateMailed/
Given
DateRec’d
DIVISIONOFNUTRITION
ApptDate WICID#
Street:___________________________________
_
Apt:______
_
Zip:_________________
Phone:()________‐_______
_
OnWICBefore:Yes□ No□
MaidenName:____________________________________________
_
Date:
CurrentHeight___________inches
City: Zip:
Fax#:
Date:
HealthCareProvider:Pleasecompletethissection.
EDD_____/_____/_____
DateofDelivery/(Termination,ifany)_____/_____/_____
Hgb______gm/dLOR Hct______%
_____/_____/_____
I authorize __________________________________________________(Health Care Provider) to release the information below to the WIC Program, and I authorize
the WIC Program to release information about me to this health care provider for the purposes of coordinating my health care. If I need to transfer to another WIC
Program,IauthorizethereleaseofthisinformationtothetransferringWICProgram.Allinformationisconsideredconfidential.
YOURSIGNATURE:___________________________________________
WEIGHTandHEIGHTmustbelessthan60daysoldonthedate
Gravida_______Para_______MultiFetal____________
ForWIC
Use:
Language(s)Spoken:__________________________________
LastName(Print):____________________________________
_
City:_____________________________
DateofBirth:______/______/______
WICMEDICALREFERRALFORMFORWOMEN
FirstName:______________________________________________
_
CurrentWeight__________pounds
_____/_____/_____
_____/_____/_____
•BloodworkmustbetakenafterdeliveryforBreastfeeding/Postpartum
Women.
BloodLead__________mcg/dL
(Optional)
PrenatalCareBegan_____/_____/_____
TotalWeightGained______poundsWeeksGestation______
CurrentInfant’sBirthWeight______lb______ozOR ______kg
_____/_____/_____
•Bloodworkmustbetakenduringcurrentpregnancy.
SPECIFICMEDICALDIAGNOSISORNUTRITIONAL/HEALTHRISKSincludingICD‐9code
PRENATALORPOSTPARTUM:
DateTaken:
oftheWICappointment:_____/_____/_____
□FetalWeight<10
th
PercentileforGestationalAge
HEMATOLOGY: BREASTFEEDING/POSTPARTUM:MostRecentPregnancy
DateTaken:
PregravidWeight__________pounds
______/______/______
SendCompletedFormTo:
DOH‐799(10/08) Thisinstitutionisanequalopportunity provider.
Provider'sName(PleasePrint):
Title:
MedicalOffice/Clinic:
Street:
Phone#:
SignatureofHealthCareProvider


