
Fillable Printable 2009 Ic-004 Form Pw-1 Wisconsin Nonresident Income Or Franchise Tax Withholding On Pass-Through Entity Income
Fillable Printable 2009 Ic-004 Form Pw-1 Wisconsin Nonresident Income Or Franchise Tax Withholding On Pass-Through Entity Income
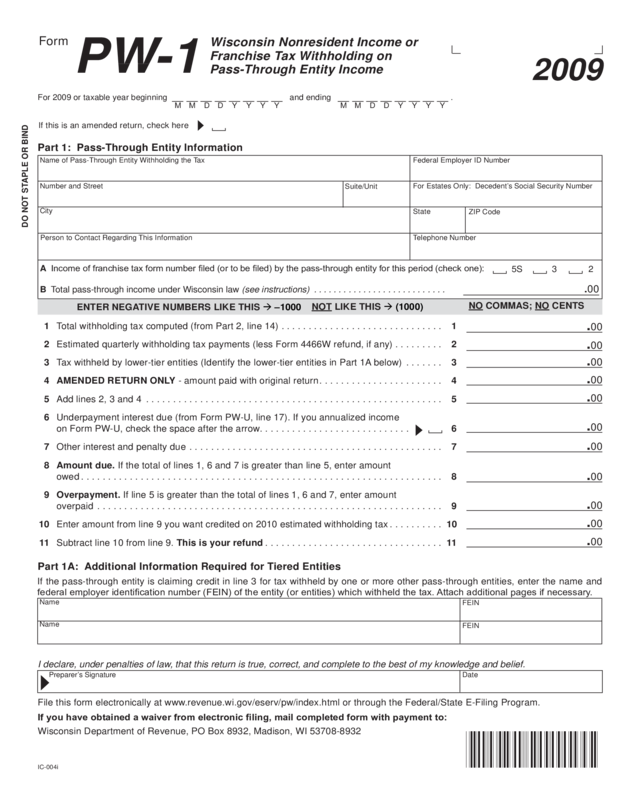
2009 Ic-004 Form Pw-1 Wisconsin Nonresident Income Or Franchise Tax Withholding On Pass-Through Entity Income
2009
PW-1
Wisconsin Nonresident Income or
Franchise Tax Withholding on
Pass-Through Entity Income
Form
IC-004i
For 2009 or taxable year beginning and ending .
If this is an amended return, check here
M Y Y Y Y D D M
M Y Y Y Y D D M
DO NOT STAPLE OR BIND
Part 1: Pass-Through Entity Information
Name of Pass-Through Entity Withholding the Tax
Federal Employer ID Number
For Estates Only: Decedent’s Social Security Number
Number and Street
City
State
ZIP Code
Person to Contact Regarding This Information
Telephone Number
5S
3 2
1 Total withholding tax computed (from Part 2, line 14) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Estimated quarterly withholding tax payments (less Form 4466W refund, if any) . . . . . . . . . 2
3 Tax withheld by lower-tier entities (Identify the lower-tier entities in Part 1A below) . . . . . . . 3
4 AMENDED RETURN ONLY - amount paid with original return . . . . . . . . . . . . . . . . . . . . . . . 4
5 Add lines 2, 3 and 4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
6 Underpayment interest due (from Form PW-U, line 17). If you annualized income
on Form PW-U, check the space after the arrow. . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
7 Other interest and penalty due . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
8 A
mount due. If the total of lines 1, 6 and 7 is greater than line 5, enter amount
owed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
9 O
verpayment. If line 5 is greater than the total of lines 1, 6 and 7, enter amount
overpaid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
1
0 Enter amount from line 9 you want credited on 2010 estimated withholding tax . . . . . . . . . . 1
0
11 Subtract line 10 from line 9. This is your refund . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1
.00
.00
.00
.00
NO COMMAS; NO CENTS
NOT LIkE ThIS (1000)
ENTER NEgATIvE NUMBERS LIkE ThIS –1000
.00
.00
.00
.00
.00
.00
.00
Part 1A: Additional Information Required for Tiered Entities
If you have obtained a waiver from electronic ling, mail completed form with payment to:
Wisconsin Department of Revenue, PO Box 8932, Madison, WI 53708-8932
If the pass-through entity is claiming credit in line 3 for tax withheld by one or more other pass-through entities, enter the name and
federal employer identication number (FEIN) of the entity (or entities) which withheld the tax. Attach additional pages if necessary.
Name
Name
FEIN
FEIN
I declare, under penalties of law, that this return is true, correct, and complete to the best of my knowledge and belief.
Preparer’s Signature Date
A Income of franchise tax form number led (or to be led) by the pass-through entity for this period (check one):
B Total pass-through income under Wisconsin law (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . .
.00
File this form electronically at www.revenue.wi.gov/eserv/pw/index.html or through the Federal/State E-Filing Program.
Suite/Unit
IC-004
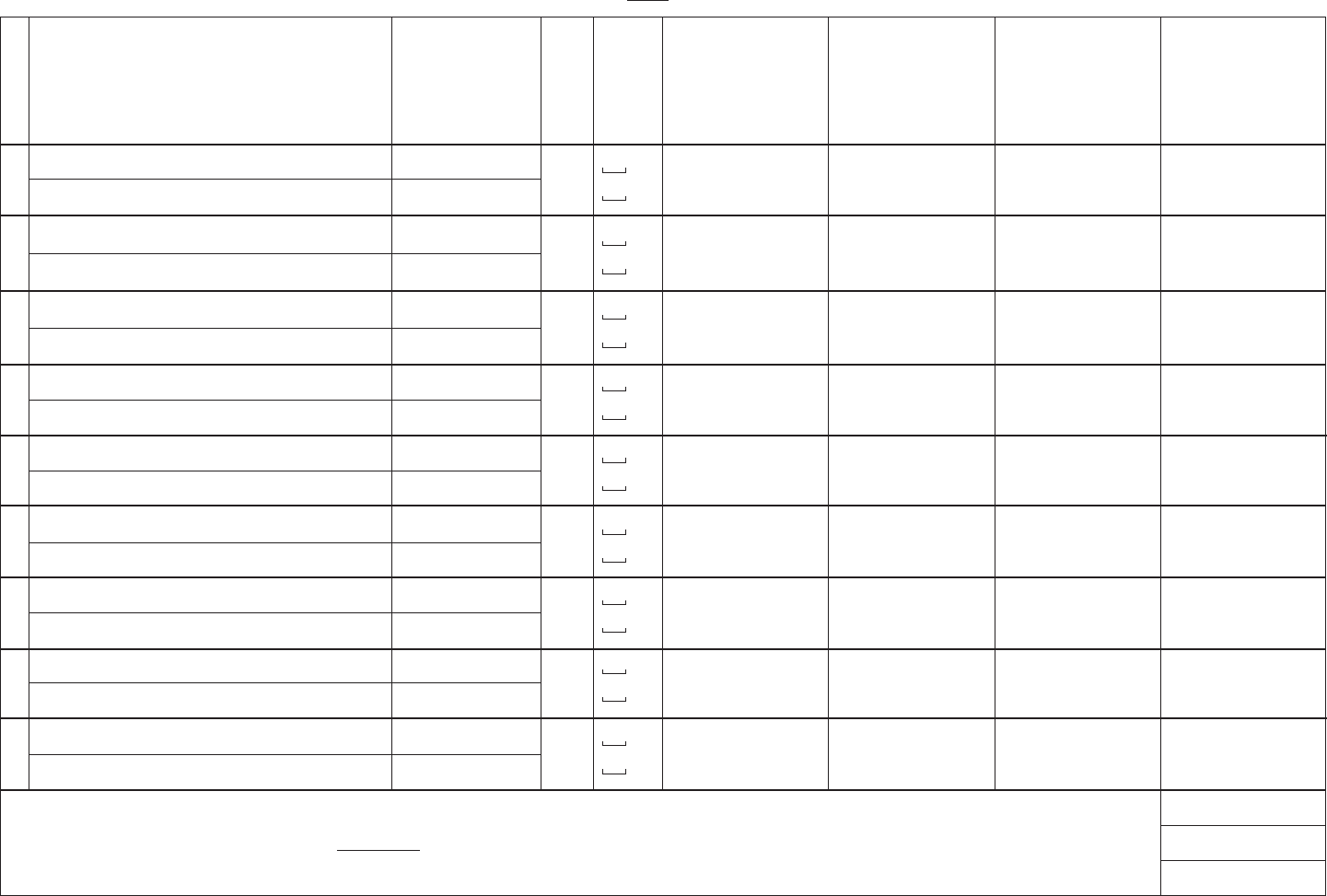
(Note: See instructions corresponding to each column letter)
Part 2: Nonresident Shareholder, Partner, Member, or Beneciary Information
A.
Nonresident’s Name and Address
L
i
n
e
H.
Withholding
Tax
Computed
F.
Gross
Withholding
E.
Share of
Wisconsin
Taxable
Income
D.
Afdavit
Filed
C.
Tax
Form
B.
FEIN or SSN
If afdavit (Form PW-2) was led by nonresident, columns E through H are not required.
a
b
c
d
e
h
f
12 Total withholding this page . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13 N
umber of additional pages included . Total of line 12 amount from all additional pages . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14 T
otal withholding tax computed. Add lines 12 and 13. Enter total on Part 1, line 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
g
i
Name
Address
Name
Address
Name
Address
Name
Address
Name
Address
Name
Address
Name
Address
Name
Address
Name
Address
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
FEIN
FEIN
SSN
SSN
FEIN
SSN
FEIN
SSN
FEIN
SSN
FEIN
SSN
FEIN
SSN
FEIN
SSN
FEIN
SSN
$
$
$
$
$
$
$
$
$
Yes
No
Yes
No
Yes
No
Yes
No
Yes
No
Yes
No
Yes
No
Yes
No
Yes
No
G.
Share of
Tax Credits
$
$
$
$
$
$
$
$
$


