
Fillable Printable Report Of Voluntary Plan Disability Claim (De 2523)
Fillable Printable Report Of Voluntary Plan Disability Claim (De 2523)
Report Of Voluntary Plan Disability Claim (De 2523)
DE 2523 Rev. 20 (8-17) (INTERNET) Page 1 of 2
CU
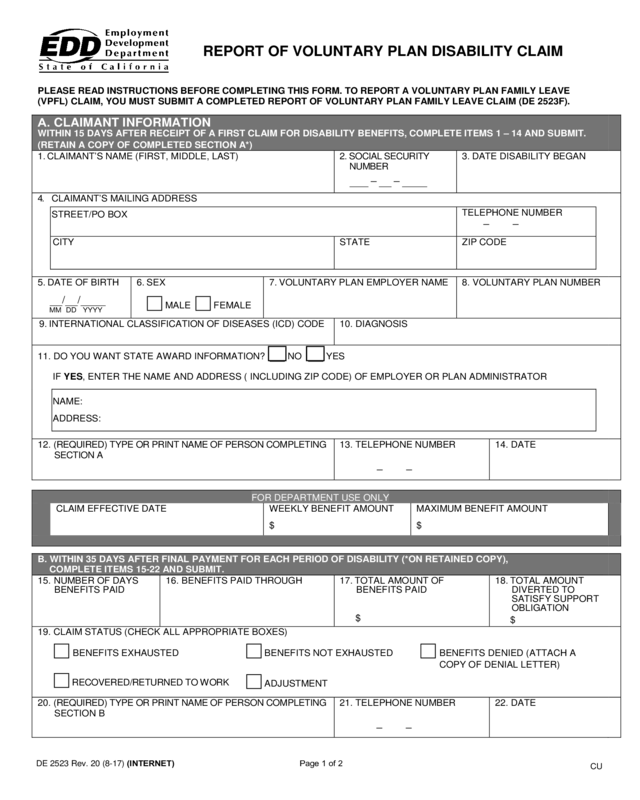
REPORT OF V O LUNTARY PLAN DISABILITY CLAIM
PLEASE READ INSTRUCTIONS BEFORE COMPLETING THIS FORM. TO REPORT A V OL UNTARY PLAN FAMILY LEAVE
(VPFL) CLAIM, YOU MUST SUBMIT A COMPLETE D RE P ORT OF VOLUNTARY PLAN FAMILY LEAVE CLAIM (DE 2523F).
A. CLAIMANT INFORMATION
WITHIN 15 DAYS AFTER RECEIPT OF A FIRST CLAIM FOR DISABILITY BENEFITS, COMPLETE ITEMS 1 – 14 AND SUBMIT.
(RETAIN A COPY OF COMPLETED SECTION A*)
1. CLAIMANT’S NAME (FIRST, MIDDLE, LAST)
2. SOCIAL SECURITY
NUMBER
– –
3.
DATE DISABILITY BEGAN
4.
CLAIMANT’S MAILING ADDRESS
STREET/PO BOX
TELEPHONE NUMBER
– –
CITY
STATE
ZIP CODE
5.
DATE OF BIRTH
/ /
MM DD YYYY
6.
SEX
MALE FEMALE
7.
VOLUNTARY PLAN EMPLOYER NAME
8. VOLUNTARY PLAN NUMBER
9.
INTERNATIONAL CLASSIFICATION OF DISEASES (ICD) CODE
10. DIAGNOSIS
11. DO YOU WANT STATE AWARD INFORMATION? NO YES
IF YES, ENTER THE NAME AND ADDRESS ( INCLUDING ZIP CODE) OF EMPLOYER OR PLAN ADMINIS TRATOR
NAME:
ADDRESS:
12. (REQUIRED) TYPE OR PRINT NAME OF PERSON COMPLETING
SECTION A
13. TELEPHONE NUMBER
– –
14. DATE
FOR DEPARTMENT USE ONLY
CLAIM EFFECTIVE DATE
W EEKLY BENEFIT AMOUNT
$
MAXIMUM BENEFIT AMOUNT
$
B. WITHIN 35 DAYS AFTER FINAL PAYMENT FOR EACH PERIOD OF DISABILI TY (*ON RETAINED COPY),
COMPLETE ITEMS 15-22 AND SUBMIT.
15. NUMBER OF DAYS
BENEFITS PAID
16. BENEFI TS PAID THROUGH
17. TOTAL AMOUNT OF
BENEFITS PAID
$
18. TOTAL AMOUNT
DIVERTED TO
SATISFY SUPPORT
OBLIGATION
$
19. CLAIM STATUS (CHECK ALL APPROPRIATE BOXES)
BENEFITS EXHAUSTED BENEFITS NOT EXHAUSTED BENEFITS DENIED (ATTACH A
COPY OF DENIAL LETTER)
RECOVERED/RETURNED TO WORK
ADJUSTMENT
20. (REQUIRED) TYPE OR PRINT NAME OF PERSON COMPLETING
SECTION B
21. TELEPHONE NUMBER
– –
22. DATE
INSTRUCTIO NS F OR COMPLETING THE
REPORT OF VO L UNTARY PLAN DISABILITY CLAIM, DE 2523
Section A: Complete items 1-14 and return within 15 days after the receipt of a first claim for disability benefits.
Submit to address below. (Retain a copy of completed Section A.) California Code of Regulation s, Title 22,
Section 326 7-1.
1. Enter the claimant’s full name.
2. Enter all digits of the claimant’s social security number.
(A claim cannot be processed without an accurate number. The use of an incorrect number can result in erroneous notices to the
claimant and employer.)
3. Enter the date the disability began.
4. Enter the claimant’s current mailing address and tele pho ne number .
5. Enter the month, day, and year of claimant’s date of birth. (mm/dd/yyyy)
6. Enter a check mark in the appropriate box.
7. Enter the employer's name.
8. Enter the six digit voluntary plan number.
9. Enter International Classification of Diseases (ICD) C ode. [Published by the World Health Organization (WHO)].
10. Enter the physician’s diagnosis.
11. Enter an “X” in the appropriate box. If yes is checked, the EDD will mail the award information to the address provided.
12. Enter the printed name of the person completing Section A.
13. Enter the telephone number of the person completing Section A.
14. Enter the current date.
Sectio n B: On the retained copy of Section A, complete items 15-22 and return within 35 days after final
payment for each period of disability, California Code of Regulations, Title 22, Sect ion 326 7-1. Submit to
address below.
15. Enter the number of days disability benefits were paid.
(Includes days paid under a supplemental accident and sickness plan or salary continuance only if they are part of the
Voluntary Plan.)
16. Enter the last date for which disability benefits were paid.
17. Enter the amount of disability benefits paid.
(Enter the amount paid for the days entered in item 15. Include any amount withheld for support obligation.)
18. Enter the amount of disability benefits that were diverted to satisfy a support obligation.
(Enter the amount of benefits withheld under the Support Intercept Program. This amount must be included in the total of item 17.)
19. Enter an “X” in the boxes that apply to the current claim stat us.
Benefits Exhausted: The total maximum benefit amount paid.
Benefits Not Exhausted: A balance of the maximum benefit amount remains.
Benefits Denied: No benefits have been paid. A copy of the denial letter to the claimant must be electronically attached or
submitted under separate cover.
Recovered/R eturn to Work: The claimant has recovered from the disability and/or returned to work.
Adjustment: Use i f submitting an amended report.
20. Enter the printed name of the person completing Section B.
21. Enter the teleph one number of the person completing Section B.
22. Enter the current date.
INTERNET or HARDCOPY VERSION/SUBMIT COMPLETED FORM AS FOLLOWS:
MAIL TO:
FAX TO:
Employment Development Department
Voluntary Plan Unit
PO Box 120831
San Diego, CA 92112-0831
916-449-1922
DE 2523 Rev. 20 (8-17) (INTERNET) Page 2 of 2


