
Fillable Printable Form 245-037-000
Fillable Printable Form 245-037-000
Form 245-037-000
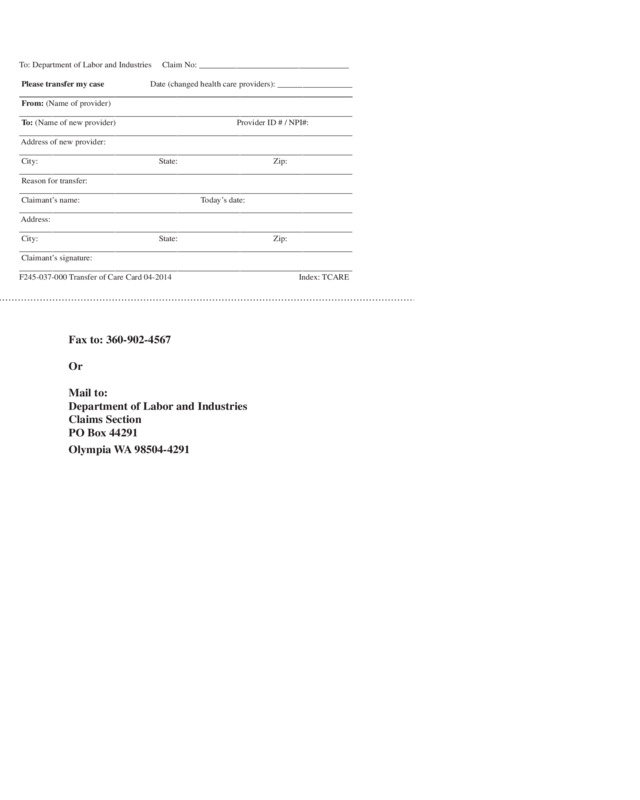
To: Department of Labor and Industries Claim No: ____________________________________
Please transfer my case Date (changed health care providers): __________________
________________________________________________________________________________
From: (Name of provider)
________________________________________________________________________________
To: (Name of new provider) Provider ID # / NPI#:
________________________________________________________________________________
Address of new provider:
________________________________________________________________________________
City: State: Zip:
________________________________________________________________________________
Reason for transfer:
________________________________________________________________________________
Claimant’s name: Today’s date:
________________________________________________________________________________
Address:
________________________________________________________________________________
City: State: Zip:
________________________________________________________________________________
Claimant’s signature:
________________________________________________________________________________
F245-037-000 Transfer of Care Card 04-2014 Index: TCARE
Fax to: 360-902-4567
Or
Mail to:
Department of Labor and Industries
Claims Section
PO Box 44291
Olympia WA 98504-4291
RESET


