
Fillable Printable 2015 Ic-005 Form Pw-2 Wisconsin Nonresident Partner, Member, Shareholder, Or Beneficiary Withholding Exemption Affidavit
Fillable Printable 2015 Ic-005 Form Pw-2 Wisconsin Nonresident Partner, Member, Shareholder, Or Beneficiary Withholding Exemption Affidavit
2015 Ic-005 Form Pw-2 Wisconsin Nonresident Partner, Member, Shareholder, Or Beneficiary Withholding Exemption Affidavit
2015
PW-2
Wisconsin Nonresident Partner,
Member, Shareholder, or Beneciary
Withholding Exemption Afdavit
Form
IC-005
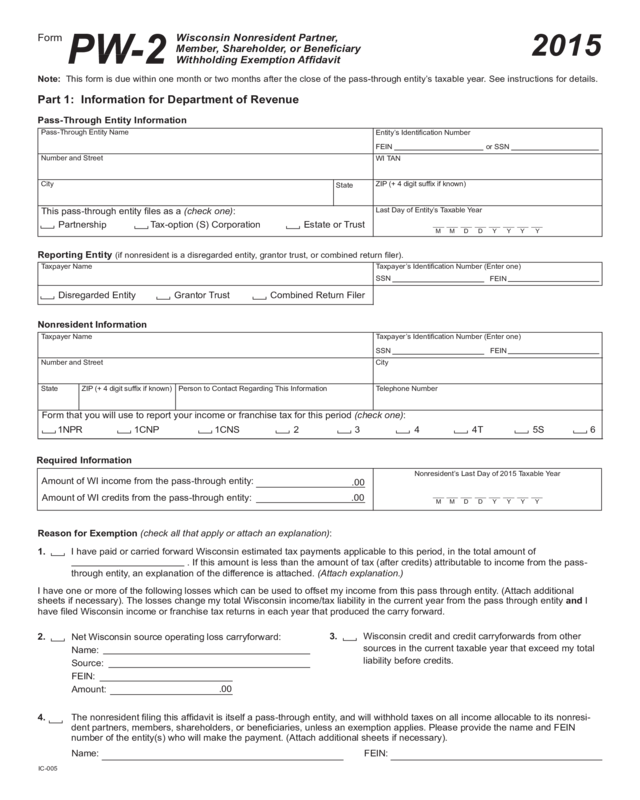
Note: This form is due within one month or two months after the close of the pass-through entity’s taxable year. See instructions for details.
Part 1: Information for Department of Revenue
Pass-Through Entity Information
Pass-Through Entity Name
Number and Street
State
ZIP (+ 4 digit sufx if known)
This pass-through entity les as a (check one):
Entity’s Identication Number
WI TAN
FEIN or SSN
Last Day of Entity’s Taxable Year
M Y Y Y Y
M
D D
Partnership
Tax-option (S) Corporation
Estate or Trust
City
Reporting Entity (if nonresident is a disregarded entity, grantor trust, or combined return ler).
Taxpayer Name
Taxpayer’s Identication Number (Enter one)
FEIN
SSN
Number and Street
State ZIP (+ 4 digit sufx if known)
Form that you will use to report your income or franchise tax for this period (check one):
Nonresident Information
City
Telephone Number
Taxpayer Name
Taxpayer’s Identication Number (Enter one)
FEIN
SSN
Person to Contact Regarding This Information
1NPR 1CNP 1CNS 2 3
4 6
5S
4T
Amount of WI income from the pass-through entity:
Nonresident’s Last Day of 2015 Taxable Year
Amount of WI credits from the pass-through entity:
M
Y Y
Y
Y
M
D
D
.00
.00
Disregarded Entity
Grantor Trust
Combined Return Filer
4. The nonresident ling this afdavit is itself a pass-through entity, and will withhold taxes on all income allocable to its nonresi-
dent partners, members, shareholders, or beneciaries, unless an exemption applies. Please provide the name and FEIN
number of the entity(s) who will make the payment. (Attach additional sheets if necessary).
Reason for Exemption (check all that apply or attach an explanation):
1. I have paid or carried forward Wisconsin estimated tax payments applicable to this period, in the total amount of
. If this amount is less than the amount of tax (after credits) attributable to income from the pass-
through entity, an explanation of the difference is attached. (Attach explanation.)
I have one or more of the following losses which can be used to offset my income from this pass through entity. (Attach additional
sheets if necessary). The losses change my total Wisconsin income/tax liability in the current year from the pass through entity and I
have led Wisconsin income or franchise tax returns in each year that produced the carry forward.
2.
Net Wisconsin source operating loss carryforward:
Name:
Source:
FEIN:
Amount:
.00
3.
Wisconsin credit and credit carryforwards from other
sources in the current taxable year that exceed my total
liability before credits.
Name: FEIN:
Required Information
2015
PW-2
Wisconsin Nonresident Partner,
Member, Shareholder, or Beneciary
Withholding Exemption Afdavit
Form
Part 2
Part 2: Information for Department of Revenue and Pass-Through Entity
Agreement to File, Routing, Declaration, and Signature
I, ,asanonresidentpartner,member,shareholder,orbeneciaryofthe
pass-throughentity ,requestthispass-throughentitytobeexemptfrom
theWisconsinincomeorfranchisetaxwithholdingrequirementfoundinsec.71.775,Wis.Stats.,formytaxyearending
.
BysigningthisafdavitIagreetotimelyleaWisconsinincomeorfranchisetaxreturnformytaxyearshownabove.
IagreetobesubjecttothepersonaljurisdictionoftheWisconsinDepartmentofRevenue,theWisconsinTaxAppeals
Commission,andthecourtsofthisstateforthepurposeofdeterminingandcollectinganyWisconsintaxes,including
estimatedtaxpayments,togetherwithanyinterestandpenalties.
The Department will return this form by mail. Enter address information below. Please type or print legibly.
Number and Street
State
To Attention of
City
ZIP Code
Company Name (if applicable)
Send Parts 1 and 2 of this form to the Wisconsin Department of Revenue at:
Fax: (Use cover page provided with instructions)
Mail: Wisconsin Department of Revenue
BTS/PTE, Mail Stop 3-107
PO Box 8958
Madison, WI 53708-8958
The Department will return Part 2 of Form PW-2 to you within approximately 30 days of receiving it. If the Department has
approved Form PW-2, provide this page to the pass-through entity. The pass-through entity must keep a copy of this page
for its records as documentation showing why it did not pay withholding tax on your behalf.
Approval by Department of Revenue
Approved for 2015 Taxable Year
Date
Reviewer’s Initials
Not Approved
Ideclarethattheinformationprovidedinthisafdavitiscompleteandaccurate,andthatImeetallrequirementsoftheexemption
checkedinPart1.IunderstandthattheDepartmentwillreturnPart2ofthisformtome.Ifurtherunderstandthatapprovalofthis
afdavitdoesnotconstituteanauditbytheDepartment,andthattheDepartment’sdeterminationregardingapprovalofthisafdavit
may not be appealed.
Taxpayer’s Signature DateTitle (if applicable)
Third
Party
Designee
Designee’s
name
Phone
no. ( )
Personal
identication
number (PIN)
Do you want to allow another person to discuss this return with the department? Yes Complete the following. No


